Atelectasis

You've just intubated a critically ill patient in the emergency department, and you're feeling pretty heroic.
Sure, it took you a little while to navigate through the secretions and blood to find the larynx, and okay the cuff needed a bit of a wiggle to get through the cords, but you got there, and the smooth square wave of the end tidal CO2 signalled your success to the world.
You've even listened to both lungs to check you haven't slid the tube in too far.
So why are the sats still dropping?
What happens normally
You and your patient have both evolved for negative pressure ventilation.
Elastic lungs hang suspended from the ribcage, with the former trying to collapse down, and the latter trying to swing open.
When relaxed, they sit at equilibrium with the lungs held open at their functional residual capacity.
This set up is very efficient, because it only takes a relatively small force to tip the scales and pull the chest wall open.
This generates a very small negative intrathoracic pressure of 2 - 5 cmH2O, and the atmosphere does the rest of the work.
As well as the energy efficient mechanism of breathing, this set up has other benefits:
- The negative intrathoracic pressure helps hold alveoli, small airways and pulmonary blood vessels open
- It also helps improve venous return from the body and head to the heart
What happens when you intubate
Three things happen when we render our patients insensible to the traumas of the real world and unable to breathe for themselves:
- They lie down (hopefully before they're unconscious)
- They lose essentially all of their muscle tone
- We switch to a positive pressure ventilatory set up once we're plugged into the ventilator
When you lie down, the physics of your thorax changes dramatically. In the same way a whale isn't designed to lie on a beach, we're not really designed to lie flat on our back.
To start with, the abdominal organs and fat press upwards on the diaphragm, making it harder for the lungs to distend caudally.
Secondly, all of the chest wall mass (and breasts if present) press directly down on the ribcage and reducing thoracic expansion further.
Thirdly, the delicate balance of 'I'll send the air to where you're sending the blood' that we call V:Q matching gets thrown out of whack, so the whole cardiorespiratory system becomes significantly less efficient.
But that's okay, we can still breathe.
Unless we can't, because someone's given us rocuronium.
- The diaphragm now loses the heavily underappreciated tonic activity that was keeping the abdominal organs at bay, and moves north
- The chest wall muscles also relax further, reducing the cross sectional area of the chest
- The spinal muscles relax which increases thoracic spinal curvature
These three factors reduce FRC by up to 20% and that's before you consider the upper airway relaxation and inevitable obstruction.
This is a large part of the reason why anaesthetised patients require more inspired oxygen than sleeping ones, especially if they're obese.
So why is this a problem?
Well if you reduce the volume of the lungs down far enough, then you run into two main issues:
- The surface area available for gas exchange is much smaller
- If you start going below closing capacity then the small airways start to close off, in a process called atelectasis
Remind me what closing capacity is
This is the volume in the thorax at which the smallest airways start to close.
It's not the volume per se that's causing the closure to occur, it's just the volume that the thorax happens to contain when this process starts to occur.
A capacity is a sum of volumes, so closing capacity is:
- Residual volume plus
- Closing volume
These are semantic definitions with no real clinical relevance.
What matters is whether your patient's closing capacity is larger or smaller than their functional residual capacity.
- If closing capacity is smaller than functional residual capacity, then the small airways will remain open when the lungs relax down to FRC and no further
- If closing capacity is larger than the FRC, we have an issue
- As the lungs relax down to FRC, the small airways will start to close and there will be loss of gas exchange, and large chunks of the lung will become very unhelpful shunt
When you lie flat on your back, closing capacity is lower than FRC until the age of 44, after which point you start to get small airway collapse in the supine position.
Standing up, CC is lower than FRC until the age of 70.
If you can spout this in a viva, then you're golden - you don't need more detail than this for an exam scenario.
So what's atelectasis?
It's Greek.
- ateles = ‘incomplete’
- ektosis = ‘extension’
And it has been used since the 1800s to describe areas of lung collapse that leads to areas of intrapulmonary shunt.
Surely my wonderful hypoxic pulmonary vasoconstriction response will save me?
Unfortunately volatile anaesthetic agents partially inhibit hypoxic pulmonary vasoconstriction, reducing the main defence against shunt.
Oops.
How does it happen?
In four main ways:
- Obstruction
- Compression
- Absorption
- Surface tension
Obstruction
- If an airway gets obstructed and can't ventilate properly, then everything downstream of that obstruction will collapse as the gas inside is gradually absorbed
- This can be a lobule, a lobe or an entire lung
Compression
- Direct compression from outside the airway physically squishes the alveoli and small airways shut
- This could be an intrathoracic mass (tumour, haematoma, abscess)
- Or an extrathoracic problem (obesity, direct external pressure)
Absorption
- All gases are not equal in their rates of absorption from the alveoli into the blood
- Nitrogen is relatively slow to diffuse, while oxygen is far quicker
- Therefore an alveolus full of pure oxygen will theoretically deflate much more quickly, and to a greater extent, than one with a decent amount of nitrogen in it
This is why some anaesthetists insist on preoxygenating with slightly less than 100% oxygen, to ward off the evil atelectatic spirits.
Surface tension
- Any stressful children's birthday party will tell you that elastic spheres inherently want to collapse
- Laplace's law tells us that smaller alveoli require a higher distending pressure to remain open than larger alveoli
- The converse is also true, meaning smaller spheres are much keener to collapse
- Alveoli have surfactant which is designed to help splint alveoli open and prevent this
So it follows that anything that makes alveoli smaller, or disrupts the layer of surfactant, is going to result in more atelectasis.
In anaesthesia, compression atelectasis from reduced FRC and absorption atelectasis from high FiO₂ are the biggest culprits.
Who is at risk?
Ah excellent, a risk factors question - break it down into patient risk factors, anaesthetic factors, and surgical factors.
Patient factors
- Obesity
- Neonate
- Elderly
- Pregnant
- Smoker
- Lung disease - ARDS or chronic lung disease
All of these patients have a larger closing capacity compared to their FRC and therefore are more prone to atelectasis.
Anaesthetic factors
- All induction agents except ketamine
- High FiO2 - effect increases above 50%
- Ineffective ventilation
Surgical factors
- Position - head down is worse than supine is worse than prone
- Cardiothoracic surgery
- Bypass
- Laparoscopic surgery
- Prolonged procedure
Why it's a problem
Well if you're trying to oxygenate a patient whose alveoli are squished shut then you're both going to have a bad time.
Instead of the diaphragm smoothly pulling the alveoli open evenly across the base of the lungs where they're most compliant, and allowing the atmosphere to gently trickle lots of lovely nitrogen (nature's CPAP) in, you're using a metal box to shove large volumes of oxygen in from the top under high pressure.
This means high-concentration oxygen distributes to the areas of the lungs that are most willing to receive it (i.e. not the closed-off bits) which not only neglects the collapsed areas, but also encourages them to close too.
Now seems like a good time to mention the four traumas of the alveolar apocalypse:
Barotrauma
- Pressure physically damages the walls of the delicate small airways
Volutrauma
- Excessive tidal volume causes overdistension of alveoli and small airways
This can occur even when airway pressures are not particularly high.
Atelectotrauma
- Repeated squishing shut and reopening is bad for alveoli
- Being open is fine
- Being squished shut isn't great for gas exchange but the alveoli don't mind all that much
- It's the repeated opening and closing that does harm
Biotrauma
- Any sort of damage or physical stress will induce some degree of inflammatory response
- This inflammation then causes further damage to the fragile walls of the alveoli and small airways
All of these cause direct harm to the respiratory engine, and that's on top of the fact that the patient is already not oxygenating as efficiently as they should be.
What to do about it
Can we not just make negative pressure ventilators?
Yup, and they look like this
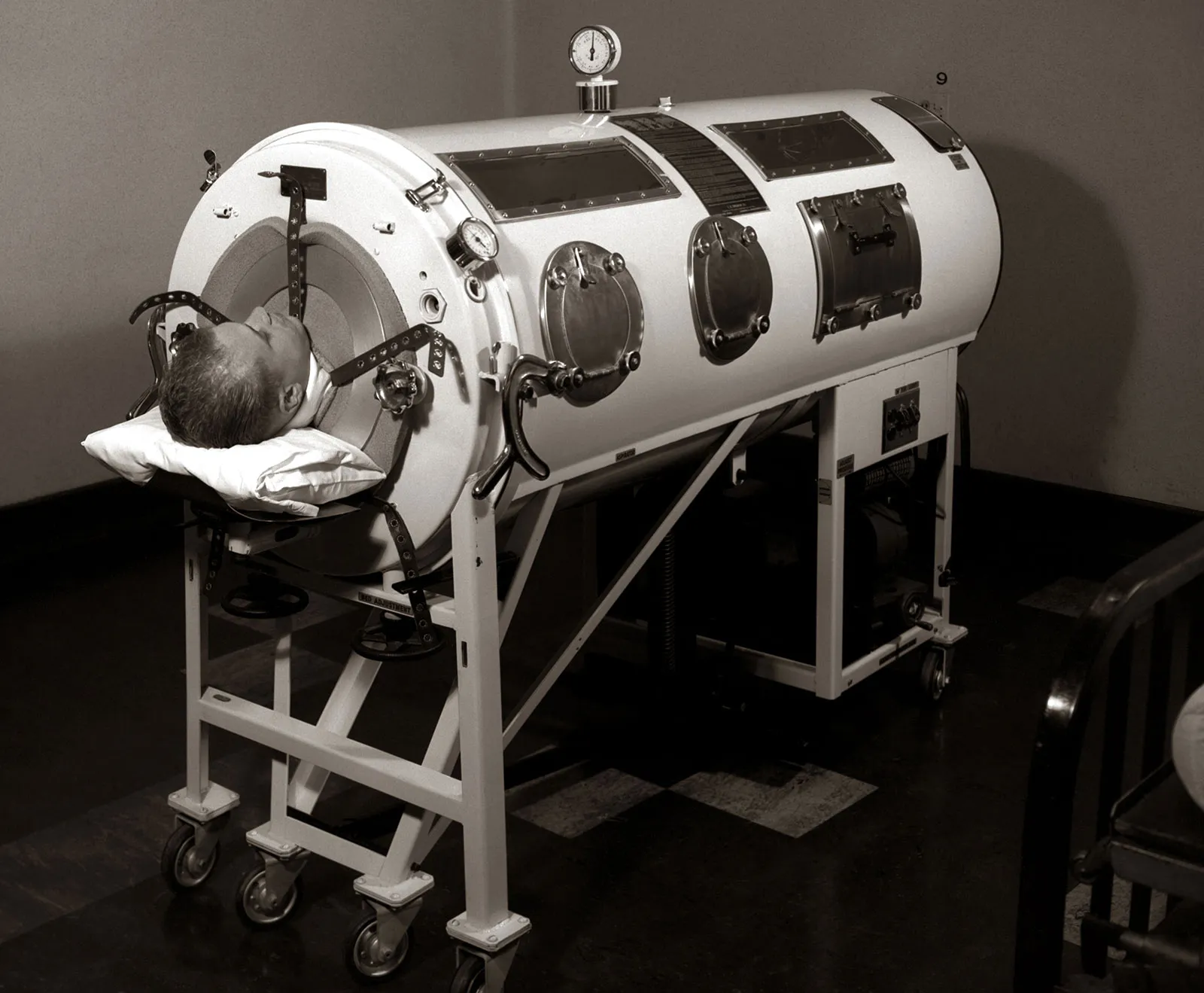
No atelectasis or access to the patient, you can only choose one.
PEEP
Positive end expiratory pressure is like pinching off a balloon before it fully deflates. The residual gas inside the balloon exerts a pressure that holds it open, and alveoli are the same.
PEEP aims to push the functional residual capacity back up above closing capacity, and keep the airways open, reducing shunt and atelectotrauma.
- Not enough PEEP - doesn't work
- Too much PEEP - volutrauma and haemodynamic compromise due to reduced venous return
FiO2
Logically speaking, leaving a little nitrogen available to splint open the alveoli if you're really worried about rapid airway collapse isn't a crazy idea.
These guys found that in 36 healthy young women, preoxygenation with 60% oxygen resulted in 97% less atelectasis, however they also desaturated twice as fast.
80% oxygen produced 87% less atelectasis, and desaturated 30% quicker.
So it seems it does genuinely have an effect, you just need to decide what scares you more - more atelectasis or less safe apnoea time.
Lung protective ventilation
This is a simple combination of reducing excessive pressure and volume inside the lungs of mechanically ventilated patients.
- 6 ml/kg predicted body weight tidal volume
- Keep the plateau pressure below 30 cmH2O
- Lowest FiO2 possible
- You can also thrown in permissive hypercapnia if the patient is really unwell, but we'll talk about that another time
It seems to be a low cost, low risk and easy way to reduce the risk of ventilator associated lung injury.
What's driving pressure?
- Driving pressure = Plateau pressure − PEEP
Increasing tidal volume will often improve oxygenation, but it does not prevent that cyclic opening and closing of alveoli that causes atelectotrauma.
Modern lung protective ventilation therefore focuses less on achieving large tidal volumes and more on minimising driving pressure.
My take home
I've written this specifically as my take home as I don't want anyone thinking I'm handing out practice-changing advice or suggesting you do it a particular way.
In my practice, I have decided that preoxygenation with the APL valve closed ever so slightly to generate around 5 cmH2O of CPAP (patients usually don't tolerate any more as they feel like they can't exhale) with an FiO2 of 90 - 95% is an adequate compromise that makes me feel like I'm warding off bad juju, both for atelectasis and safe apnoea time, without being too controversial.
If you completely disagree, please absolutely do comment or get in touch, we love a debate and are always happy to be taught something new.
References and Further Reading



Other posts


Just a quick reminder that all information posted on Anaestheasier.com is for educational purposes only aimed at trained professionals, and it does not constitute medical or clinical advice.
Anaestheasier should not be used as a definitive resource for academic writing, please reference original source material.
Anaestheasier® is a registered trademark.