A spot of history - Neuromuscular block

I've gone down a rabbit hole and insist that you join me as we dig up the dramatic, violent history of the humble neuromuscular blockade that we so take for granted in our day to day practice.
It started with poison
As many great drugs do.
- 1516 - Italian monk Peter Martyr d'Anghera describes the poison arrows used by South American natives
- These arrows were dipped in 'the stings of scorpions' and 'the juice they distil from certain trees' and apparently were so toxic that the elderly women who made them often died from inhaling the fumes (this may have been added for dramatic effect)
- 1594 - Sir Walter Raleigh visits Guyana
- His resident propagandist Richard Hakluyt wrote of his travels, and commented on the 'most ugly and lamentable death' that was induced by these weapons, and gave them the name ourari
There were at different times around 20 different but similar-sounding names for this deadly poison, all seemingly trying to use the native Amazonian word uirary which combined uira (bird) and ary (kill).
Somehow this ended up at curare, but for now we'll call it wourali, and it's essentially a haphazard concoction of plant alkaloids.
The evil duo
- If you make wourali using Chondrodendron tomentosum then the active ingredient is d-tubocurarine
- If you use Strychnos toxifera then the active chemical is the alkaloid toxiferene
Just in case you were planning on going hunting this weekend.
Unfortunately, the explorers being largely from Spain, Portugal and England all got rather distracted by a bunch of wars for a few hundred years, so exploration and understanding of these magical poison arrows largely stalled for a while until the 1800s.
Edward Bancroft, an American physician, spent a merry five years in South America and brought back samples of crude curare for examination and experimentation.
British surgeon Sir Benjamin Brodie used some of Bancroft's stash to show that small animals could be kept alive after being injected with curare by inflating their lungs with bellows, suggesting that the concoction was killing the poor creatures by inducing respiratory arrest.
Apparently the best, most murderous wourali was made by the Macushi tribe in south Guyana near Brazil.
- 1812 - Charles Waterton, naturalist and explorer, travels 400 miles up the Demerara and Essequibo rivers to collect as many samples as possible from the natives
They would take a vine called urari, cut its bark into shavings and make an aqueous extract, add a bunch of other ingredients and then boil it down to a concentrate over a ceremonial fire.
- This vine has since been identified as Strychnos toxifera
- At the time, people poisoned by these arrows seemed to have dramatic convulsive deaths, rather than the quiet paralytic demise one would expect from neuromuscular blockade. This might be due to contamination with strychnine from the Strychnos toxifera root
Waterton tested the concoction on small mammals and birds and noted that it 'manifests itself by an apparent unwillingness of the bird to move'.
He also tried it on a 250 kg ox, which took three arrows before it succumbed, in a rather crude demonstration of weight-adjusted dosing.
He also noted that the flesh of the animals was perfectly delectable and clearly it was safe to eat an animal that had been poisoned by wourali.
Three men and three donkeys
The year is 1814, and the three men are:
- Charles Waterton, our wourali-gathering explorer
- Benjamin Brodie, our surgeon of small-mammal-ventilatory fame
- Joseph Banks, explorer and Charles Waterton's mentor
These three men took three unfortunate donkeys and performed a rather brutal but scientifically elegant experiment.
Donkey number 1 received a shot of wourali to the shoulder, and promptly died around 10 minutes later.
Donkey number 2 received a tourniquet to the upper limb, and a shot of wourali distal to the tourniquet. It wandered around none the wiser until they took the tourniquet off and it, too, collapsed minutes later.
Donkey number 3, also a recipient of a shot to the shoulder, collapsed after a similar time period as the first donkey, but then received an emergency tracheotomy and artificial ventilation with a pair of bellows.
For two hours.
After which the donkey perked up and started looking around.
So they stopped ventilating it.
And it collapsed in a heap again, requiring two more hours of ventilation until finally it got to its feet and starting wandering around in no apparent distress.
Boom, proof that it's causing death through asphyxiation, and conveniently leaving the heart unscathed.
- 15th February 1839 (25 years later) - the donkey, called Wouralia, finally breathes her last after a happy comfortable life in the countryside
"It affects the nervous system and thus destroys vital functions; it is also said to be harmless provided it does not touch the blood."
Location location location
The next step was to figure out exactly where along the neuromuscular highway the drug was acting.
- 1846 - Claude Bernard sticks a ligature on a frog's leg artery in the first isolated limb experiment, and demonstrates that the drug is having an effect on the motor nervous system but not the sensory component (the isolated leg twitched when he jabbed another area of the body that was paralysed)
- He then figured out it was specifically acting at the neuromuscular junction, rather than the nerve or muscle tissue in isolation
- 1921 - Otto Loewi shows that vagal stimulation produces a chemical neurotransmitter (later identified by Dale as acetylcholine) which at the time he imaginatively called "Vagusstoff"
- It was at this point everybody realised just how awful it was to die from curare poisoning
"within the still body and staring death like eyes, feeling and intelligence persist strongly. His consciousness persists whilst his organs die one by one, imprisoned within a cadaver."
Yikes.
- By the mid-1930s Dale and colleagues had established acetylcholine as the neurotransmitter at the neuromuscular junction, and that intra-arterial injection of acetylcholine induces muscle contraction, and then in 1936 they showed that curare stops this from happening
So now we finally know how curare works - over 500 years after we start using it to kill each other.
From concoction to chemical
It's all well and good knowing that you have an incredibly potent muscle relaxant that has potentially profound implications for anaesthesia, but it's not much use when you have to boil up a bunch of tree bark and dip a spear head in it in order to use it.
You'd get some looks from passers by if you started doing this in ED.
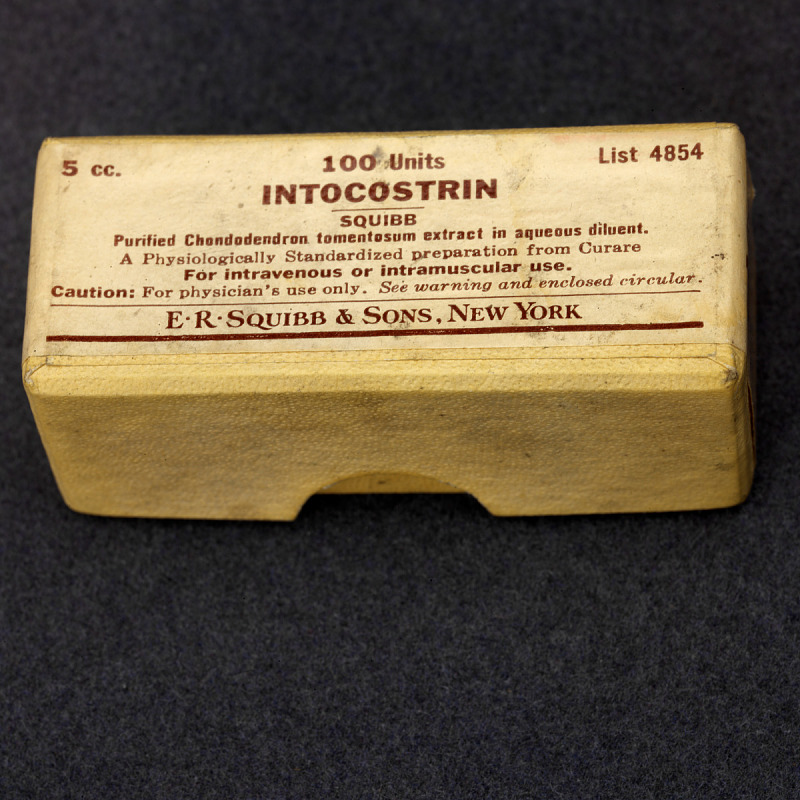
It wasn't until 1935 when the active molecule tubocurarine was isolated from curare by Harold King (from a different plant Chondrodendron tomentosum from Western Brazil and Peru)
- Tubocurarine or d-tubocurarine, is a non-depolarising muscle relaxant
- It is a bulky rigid molecule with two quaternary ammonium groups at either end (much like suxamethonium)
Brave and/or insane Dr Frederick Prescott of the Wellcome Research Institute was voluntarily injected with d-tubocurarine and ventilated to keep him alive.
His colleagues ripped plasters from his body to test its analgesic properties, of which there were none.
Why this was game changing
23 January 1942 in Montreal, Harold Randall Griffith and his resident Enid Johnson used d-tubocurarine (Intocostrin) during an appendicectomy.
This was the first deliberate use of a neuromuscular blocking drug in anaesthesia.
Griffith and Johnson reported:
‘Every anaesthetist has wished at times that he might be able to produce rapid and complete muscular relaxation in resistant patients under general anaesthesia'.
Ever tried tubing an adult on sevoflurane alone?
Well imagine how deep you'd have to get a patient on ether to get sufficient muscle relaxation for major abdominal surgery - none of this 'is the patient relaxed enough?' rubbish of today's anaesthesia - oh, and that's with no monitoring other than your finger on the pulse.
The reason muscle relaxation was such an incredible addition to the arsenal of the anaesthetists of the time is because it allowed for balanced anaesthesia.
We now had our sacred triad:
- Hypnosis
- Analgesia
- Muscle relaxation
At last, depth of sedation and muscle relaxation could be managed separately, allowing for much safer, shallower depths of anaesthesia while still keeping the patient nice and still for the surgeon.
The Liverpool Technique
- Dr John Halton was an anaesthetist in Liverpool in the 1940s
- He persuaded an American friend of his who was in the bomber squadron to bring Intocostrin over from the US
- Halton and Cecil Gray then used it on patients and were terribly pleased with the results
- Their documented triad of narcosis, analgesia and muscle relaxation was the basis of our beloved triad that we still use today
Enter the synthetics
In classic human style, thinking 'we can do better', we started work on developing synthetic versions of the drug.
Why?
Tubocurarine had several main drawbacks:
- Potency varied wildly depending on its preparation
- It had a long duration of action, lasting up to several hours
- It caused a whole load of histamine release, adding the hassle of flushing, bronchospasm, tachycardia and hypotension to an already chaotic anaesthetic
- It also blocked autonomic ganglia due to its lack of selectivity for the neuromuscular junction, making patients cardiovascularly 'wobbly' shall we say
Gallamine
- Daniel Bovet of the Pasteur Institute in Paris, started building big curare-esque molecules
- In 1947 he threw together gallamine, a trisquaternary compound that became the first clinically employed synthetic muscle relaxant
- Reliable production
- Not very selective for the neuromuscular junction, so you got autonomic side effects including profound tachycardia
- Reversible with anticholinesterases (non-depolarising competitive inhibitor of the NMJ)
Pancuronium
- 1964 Hewett and Savage built an aminosteroid with two quaternary ammonium groups
- They essentially stuck two acetylcholine molecules onto a rigid steroid-ish frame
- Their awesome theory was you needed the quaternary ammonium groups to be a certain distance apart
- And it worked
- Potent, more predictable and less histamine-releasing than tubocurarine thanks to its increased selectivity for the neuromuscular junction
- However it still had a very long duration of action and did still cause vagal blockade and tachycardia
Vecuronium
- 1975, Savarese and Kitz wanted to do better than pancuronium
- They intended to make a short, non-accumulating, non-depolarising blocker with rapid onset and recovery that could be reversed and had minimal side effects
- Instead they made vecuronium, which was slow onset with an intermediate action, but had far fewer cardiac side effects than pancuronium, to give them their due
- They also created mivacurium
- This ester-linked benzylisoquinoline is metabolized by plasma cholinesterase and has a short duration of action but still a slow onset
Atracurium
- Taking a slightly different tack, Stenlake and colleagues tried to make a muscle relaxant that would spontaneously break down via Hofmann elimination
- This would then be organ-independent and much safer in patients with renal and hepatic failure
- In 1981 they made atracurium, a benzylisoquinolinium like tubocurarine
- (This just means it has a benzene ring attached to an isoquinoline ring, like tubocurarine, papaverine and morphine)
- It breaks down completely and irreversibly at physiological pH and temperature
- It causes nondepolarizing muscle relaxation
- Slow onset and intermediate duration of action
- Ten stereoisomers can be distilled down to pure cis-atracurium for a more potent, less histaminergic version
What about Suxamethonium?
The problem with the existing drugs was twofold:
- They took ages to work (several minutes)
- They lasted too long
The appetite for a quick onset, quick offset muscle relaxant was high.
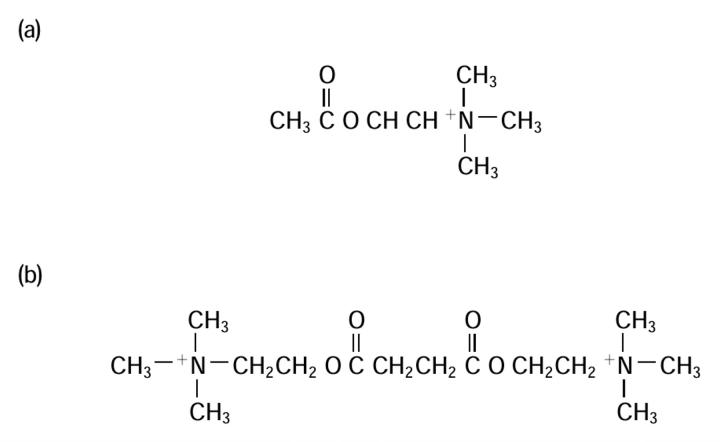
Suxamethonium or succinylcholine was the result of the beautiful scientific tradition of 'what happens if I mess around with this?' applied to acetylcholine - specifically, 'what if we join two molecules together?'.
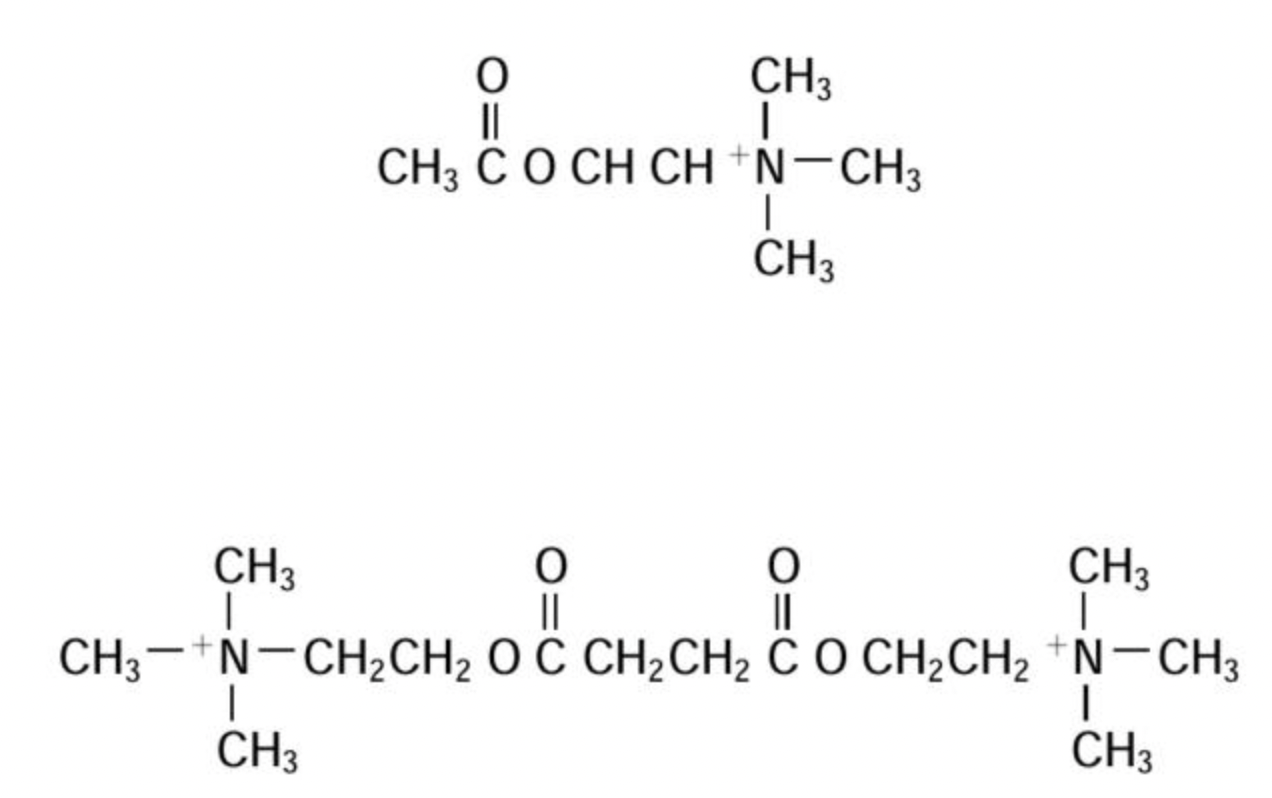
The result was rapid onset of fasciculations, followed by profound flaccid paralysis due to persistent depolarisation of the end plate, but only for a few minutes.
Bingo.
It was introduced to clinical practice in the 1950s, and quickly became the agent of choice for rapid sequence intubation thanks to its extremely rapid onset.
Bovet (going two for two) published his work on suxamethonium in 1949, and went on to win the Nobel Prize for Medicine in 1957 for his contribution to pharmacology.
However it wasn't without its own drawbacks:
- Hyperkalaemia
- Malignant hyperthermia
- Bradycardia
- Raised intraocular pressure (albeit transient)
Plus there's always the pseudocholinesterase deficiency lottery, where it might take hours to wear off.
Despite these fairly substantial downsides, it still remained the go-to for intubation for shorter procedures, as nothing else came close in terms of speed.
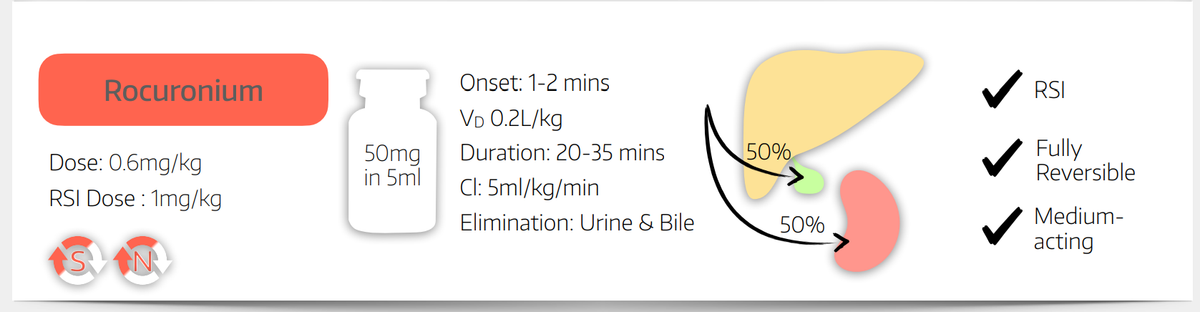
Sux sucks, Roc rocks
While sux was discovered through physiological curiosity around acetylcholine, rocuronium was the product of deliberate medicinal chemistry.
They already had the brilliant-but-slow pancuronium and vecuronium as a starting block, they just needed to speed things up a little.
- 1988 Bowman found that speed of onset relates to potency
- The more potent, the slower it kicks in
- This is because you're giving fewer molecules in the first place, so there's a smaller concentration gradient, and slower onset
- Conversely, if you give a massive dose of a less potent drug, the enormous concentration gradient gets the molecules to the active site quicker
By messing with the structure of vecuronium, they managed to craft a faster onset, intermediate-duration analogue that is almost as quick as suxamethonium.
A brief nod to Rapacuronium
Included for completeness to satisfy the author's neuroticism, Rocuronium's little sister rapacuronium was actually faster than Roc.
However it caused such fatally terrible bronchospasm sufficiently frequently that it lost its FDA approval less than two years after it joined the workforce.
You can read its tragically short Wikipedia entry here should you feel so inclined.
Rapid Onset veCURONIUM (not technically confirmed as the official origin for the name) joined the anaesthetic battlefront in the 1990s, providing smooth, reliable and speedy intubating conditions with cardiovascular stability and none of the side effects of suxamethonium.
The only problem was undoing it.
The reversal problem
For decades anaesthetists just assumed that patients had recovered sufficiently once they could lift their head off the bed for a few seconds or squeeze a hand with a decent amount of force.
Quantitative monitoring later showed many patients were still significantly paralysed in recovery, leading to respiratory complications and a whole host of unnecessary suffering.
The only depolarising agent in common practice, suxamethonium, wore off so quickly as to not really cause any issues, (assuming your pseudocholinesterases were working).
But all of the non-depolarising agents took a decent while to wear off, so if the operation was done in five minutes, you were sat waiting around for potentially hours to go home.
We'd known since the 1920s that acetylcholine was involved in muscle contraction, and that muscle relaxants interfered with this process as part of their mechanism of action.
It wasn't long until we were using neostigmine, the intermediate-acting acetylcholinesterase inhibitor to increase concentrations of acetylcholine at the NMJ and outcompete the drug in an attempt to reverse its action.
But the lack of specificity of neostigmine's action meant acetylcholine started building up everywhere, including the autonomic system, producing profoundly unpleasant side effects:
- Bradycardia
- Bronchospasm
- Salivation
Hence it needs to be given with an antimuscarinic chaser, such as glycopyrrolate.
Remember this still only works for non-depolarising agents. If you were unlucky enough to have pseudocholinesterase deficiency and given suxamethonium, then it's simply a waiting game to let it wear off.
Sugammadex changes the world
Anton Bom and colleagues at Organon, working at the Newhouse research site in Scotland, developed a modified cyclodextrin molecule that worked unlike any previous reversal drug.
It joined the European market in 2008, and changed everything.
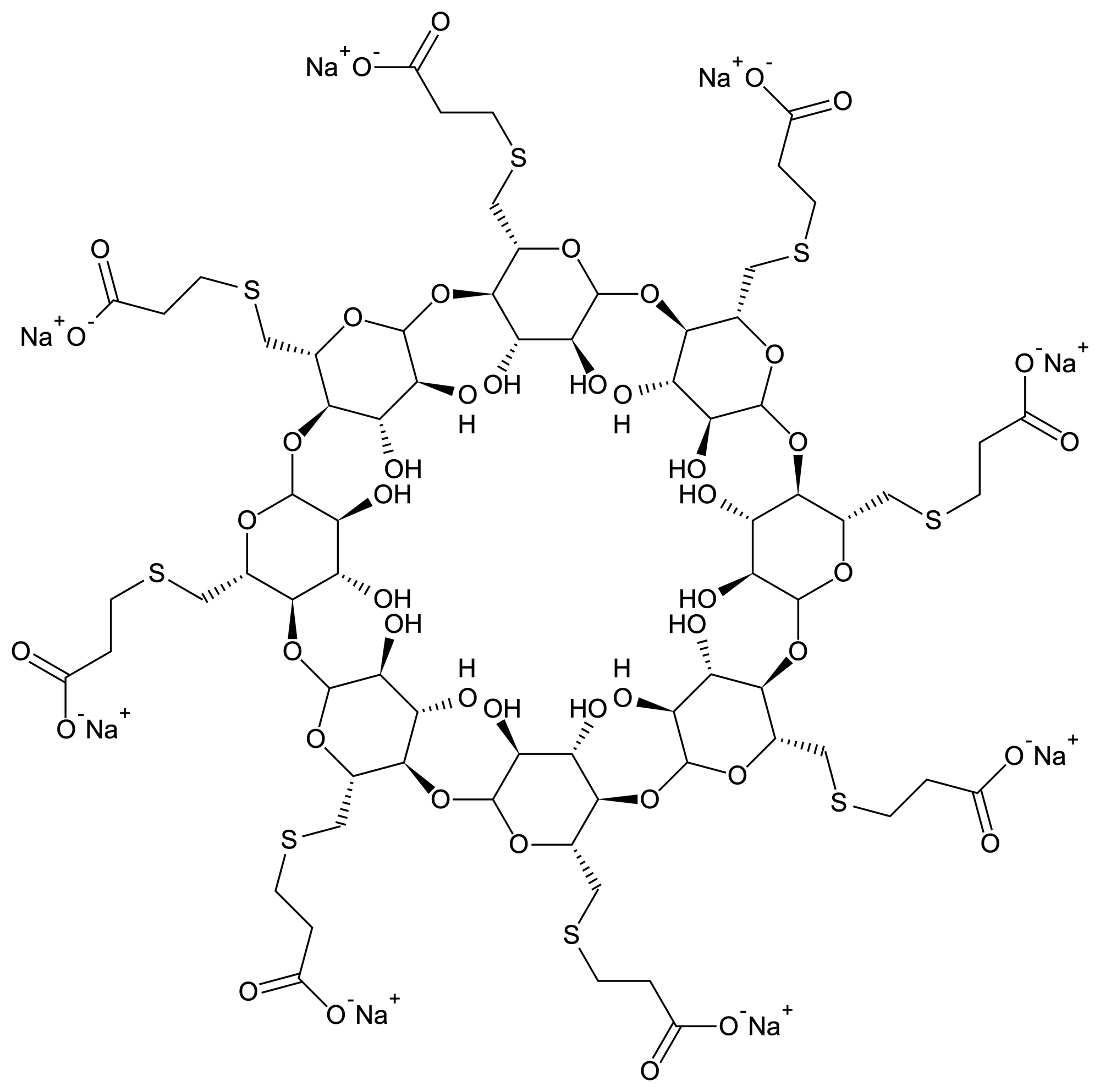
Instead of competing with the blocker for a receptor site on an enzyme or membrane channel, the cyclodextrin ring it physically encapsulates steroidal relaxants such as rocuronium and vecuronium.
One sugammadex molecule binds one relaxant molecule and immediately takes it out of the game.
For the first time ever, profound rocuronium blockade could be reversed rapidly and safely.
Sugammadex doesn't reverse neuromuscular blockade in the traditional sense by increasing acetylcholine levels or competing with it, it's even better.
After centuries of trying to outsmart curare at the receptor, we finally solved the problem by putting it in a molecular box and simply carrying it away.
So here we are
Five hundred years ago, Amazonian hunters coated arrows with a magical poison that brutally left its victims paralysed but fully conscious.
Today, we anaesthetists deliberately induce the same state of paralysis combined with hypnosis and analgesia in the patients we're looking after in order to make their anaesthetic safer.
We then reverse it minutes later with a designer molecule engineered specifically to trap the drug in a molecular cage.
THAT'S INSANELY COOL.
The journey from wourali to sugammadex is not just an interesting pharmacological journey of chemical curiosity, it's the story of how the entire field of anaesthesia realised that unconsciousness, analgesia and paralysis are not the same thing.
It has taken surgery from a barbaric Hail Mary to the beautiful, precise art form that it is today.
References and Further Reading

More History?

Coffee?

Just a quick reminder that all information posted on Anaestheasier.com is for educational purposes only aimed at trained professionals, and it does not constitute medical or clinical advice.
Anaestheasier should not be used as a definitive resource for academic writing, please reference original source material.
Anaestheasier® is a registered trademark.