Rotameters and Gas Flow
Take home messages
- Flow meters are generally classified by pressure and orifice
- Some measure flow, others measure volume, and it doesn't really matter which
- Rotameters have a whole host of safety features, which you need to know for the exam
Go with the Flow
Much of the time in our job, we give patients 'some oxygen' or 'a smidge of nitrous', and then adjust depending on the clinical picture, their observations and how unconscious they appear to be.
But it's nice to be a little more scientific at least once in a while, and actually measure exactly how much gas flow we're giving to the patient, or indeed the patient is able to breathe in and out.
Remember that whenever we measure anything in the physical world, we usually use some form of transducer.
A transducer is a device that converts energy from one form to another, and usually it's to a form that we can more easily measure or use for calculations - in our increasingly digital world, this is almost always electrical energy.
Examples:
- The pressure transducer in an arterial line converts kinetic energy of the blood into electrical energy
- A microphone converts kinetic sound energy into electrical energy
- A thermistor changes its electrical resistance depending on temperature, thereby converting heat energy into electrical energy
Pretty much all modern measuring devices do something along these lines, converting something into electrical energy, so what's particularly charming about some of the older measuring devices we discuss here is that they perform a much simpler conversion of energy, such as from the kinetic energy of the gas to the kinetic energy of a pen.
Read on.
What is flow?
Flow is simply the amount of fluid moving past a certain point in a given period of time.
Flow = volume/time
Now you can either measure flow directly, or you can measure volume and then divide it by the amount of time you spent doing the measuring, and hence we have our first FRCA question.
What are the types of devices that measure gas flow and volume?
We can immediately break this down into devices measuring volume and devices measuring flow.
We'll list the names here first, then explain how they work, because that's how you'll be expected to structure your answer in the exam.
Volume measuring devices
- Benedict-Roth Spirometer
- Vitalograph
- Wright respirometer*
*This is technically an anemometer, which measures wind speed but it uses that to calculate a volume first, and then a flow value, so it's included here.
Flow measuring devices
- Peak flow meter
- Pneumotachograph
- Rotameter
How the volume measuring types work
The Benedict-Roth Spirometer
Really simple.
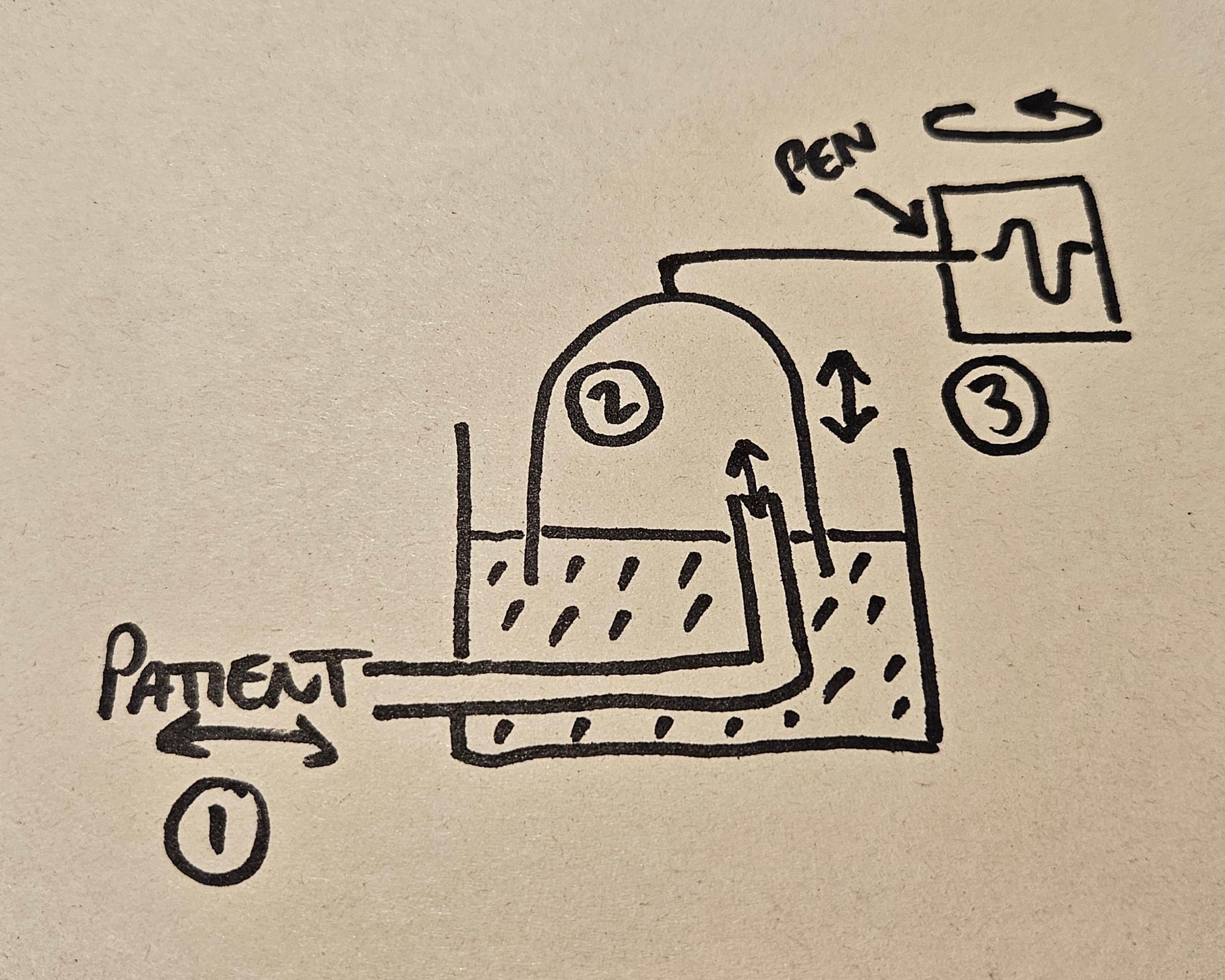
- The patient breathes in and out of a tube, the other end of which sits underneath an upside-down bell jar floating on water
- As the patient removes and adds gas to this volume, the bell jar moves up and down
- The bell jar is connected to a pen that draws a trace on a rotating drum
The trace of the pen will correspond to the change in volume, and the speed of the drum's rotation will determine how that volume changes over time, allowing you to calculate flow.
This device was mainly used to calculate the amount of oxygen consumed during quiet breathing at rest, to try and derive basal metabolic rate. (A soda lime canister prevents rebreathing and narcosis, in case you were worrying).
You do not need to know more than that for the exam, or ever really.
Vitalograph
Very similar concept here - the patient breathes in and out of a tube attached to a set of bellows that duly move up and down.
Attach a pen and slide the piece of paper across underneath it while it moves, and hey presto - a graphical representation of respiratory volumes.
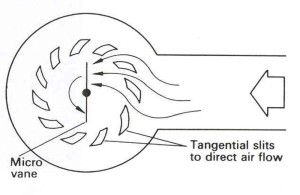
Wright respirometer
As we mentioned earlier, this is technically an anemometer, meaning that it actually measures the velocity of the gas, and then uses that to deduce a volume, and then a flow rate.
It's not overly complicated - you breath into a little fan or vane, and the faster the flow, the faster it spins. The one thing to remember is that at very high gas flows, the spinning vane has its own inertia that can cause a slight overestimate of the true flow rate.
Oh and they can only measure exhaled gas, because the fan will only spin one way.
How the flow measuring devices work
These devices directly measure the flow of gas, rather than measuring a volume and then calculating the flow.
This makes them a smidge more complex.
Peak flow meter
You've probably seen this one before.

We'll use this example to explain the whole 'pressure vs orifice' thing we mentioned a minute ago.
The patient is going to exale as hard as they can, and generate a pressure gradient across the apparatus of the flow meter. For our relatively simplistic intents and purposes, this pressure is constant, in that the pressure doesn't dramatically change across the device's mechanism during the measurement process.
The orifice in this example refers to the gaps through which the gas is able to flow, and you might have noticed that slit extending along the side of the barrel of our trusty peak flow-ometer.
At the beginning of exhalation, the gas has nowhere to go, so it forces the diaphragm to move forward along the barrel.
However as the diaphragm moves further along the barrel, this 'orifice' along the side of the barrel increases in size, allowing more gas to flow out of the side of the barrel - hence it is a variable orifice device.
There comes a point where all the gas is able to escape out of the slit, and so the diaphragm doesn’t need to move any further, giving a convenient and reliable mechanical flow measurement.
Easy - constant pressure, variable orifice
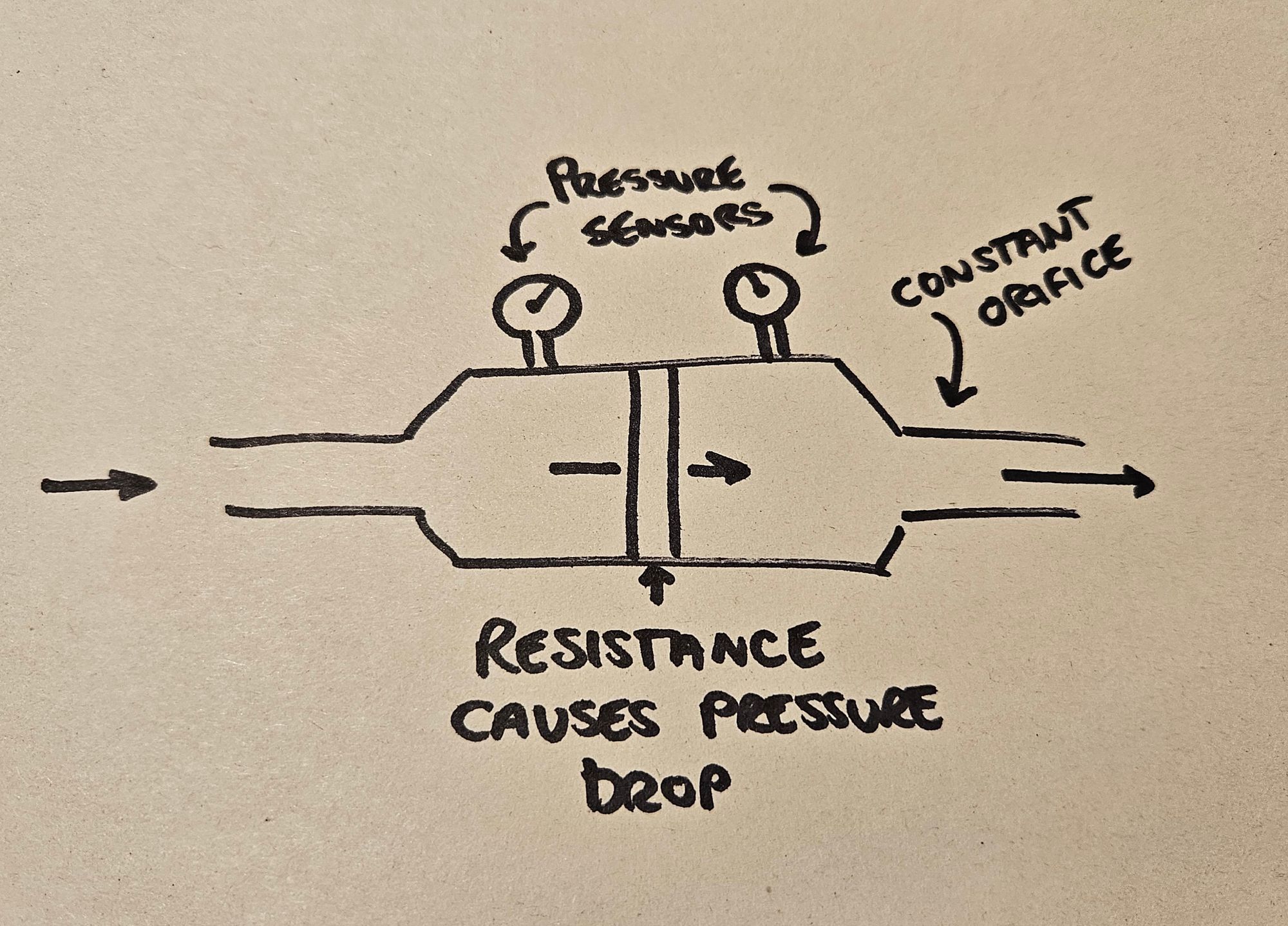
Pneumotachograph
Pneumotachographs on the other hand, are constant orifice, variable pressure devices, and they're often used in anaesthetic machines.
Instead of changing the size of the orifice, they induce a change in pressure by inserting some sort of resistance to the gas flow.
The change in pressure between the 'before' and 'after' bits of the system will vary in proportion to the change in gas flow.
This is Ohm's law again:
- Voltage = Current x Resistance
- Pressure difference = Flow x Resistance
Hence we can therefore deduce flow rate from the change in pressure we have directly measured.
There are four types you need to know about.
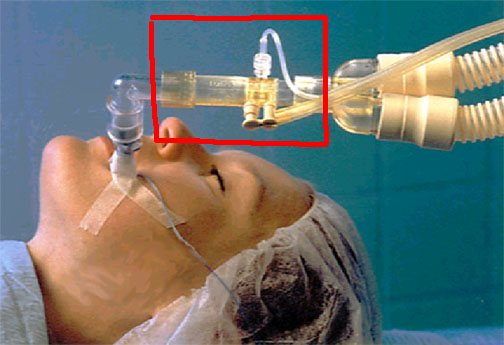
Pitot tube pneumotachograph
- Two pressure sampling tubes sit in the middle of the stream of gas
- One tube faces upstream and one downstream
- This means there will be a slight pressure difference between the two as gas flows towards one and away from the other (a bit like the Doppler effect)
- The difference in pressure will correspond to the flow rate
Pitot tubes are found in this bit of the anaesthetic breathing circuit, and they're also these little L-shaped things you see on on planes.
{kind=link}
{kind=link}
Screen pneumotachograph
- The gas flows through a screen made of gauze, which adds resistance and induces a drop in pressure depending on how fast the gas is flowing
- This pressure drop can then be measured, and calibrated to the flow rate
- Just note this requires laminar flow to work
Fleisch pneumotachograph
- This is exactly the same as the screen pneumotachograph, but instead of a screen made of gauze, it's a screen made of lots of very tiny tubes
- These tubes ensure laminar flow to give more accurate readings
Hot wire pneumotachograph
This one is a little different and runs on a completely separate principle.
- A hot wire will cool down if cold gas flows past it
- The faster the flow of gas, the greater the degree of cooling
- Therefore if you can accurately measure the temperature change then you can accurately deduce the gas flow rate, once you've calibrated the system correctly
Rotameters get their own section
Because they're super important, and really cool too.

You'll have seen these on the ward, and on older anaesthetic machines as well, and they're a simple device that runs on some beautiful physics.
The twisty dial controls a needle valve, which very precisely adjusts how much gas is allowed into the bottom of the tube.
The gas pushes upwards against a bobbin, which is usually spherical on the ward oxygen supply, and more cylindrical on an anaesthetic machine.
As the gas pushes up against the bobbin, it lifts the bobbin up the tube.
But here's the catch - the tube is actually cone shaped, getting wider further up.
This means that as the bobbin lifts up, more and more gas is able to escape around it, and so a relatively increasing amount of flow is needed to cause any further increase in bobbin height.
This is why these are constant pressure, variable orifice devices, just like the peak flow meters.
This is how you get a nice linear scale on the rotameter, rather than some weird logarithmic-looking scale that's completely impractical to use.
Now for the question that always gets asked:
What types of flow are seen at high and low flows in a rotameter?
The answer
- Laminar flow is seen at lower flows
- Turbulent flow is seen at higher flows
The explanation
- At lower flows the bobbin isn't very high up the tube, so the gap between the side of the bobbin and the tube itself is small
- Because the gap is small compared to the length of the bobbin, the gas molecules behave as if they're passing through a tube
- They therefore display laminar flow
- At faster flows the bobbin is higher up - and therefore the gap between the wall of the tube and the side of the bobbin is much larger - allowing the gas molecules to bounce around and display turbulent flow
Why is this important?
- Laminar flow is more greatly affected by the viscosity of the gas
- Turbulent flow is more greatly affected by the density of the gas
This pretty much always gets asked at some point on the anaesthetic trainees journey to FRCA freedom, so you need to know it.
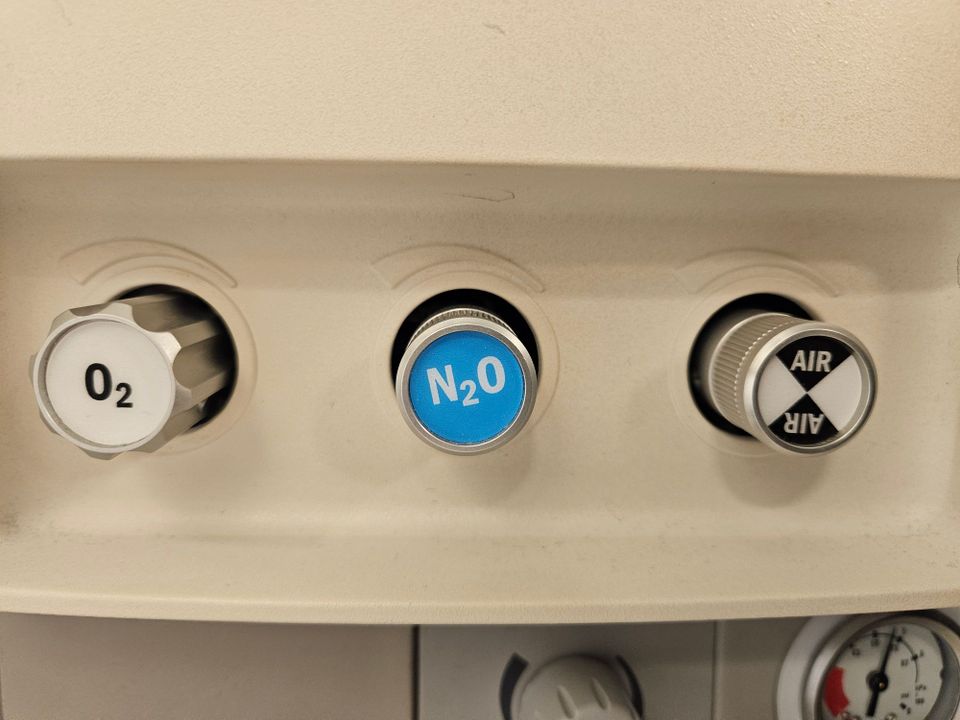
The Hypoxic Guard
Clearly if you have oxygen and nitrous oxide on separate rotameters then you could deliver a dangerously hypoxic gas mixture by only turning on the nitrous, or not enough oxygen.
To circumvent this, there is a hypoxic guard, which is a mechanical linkage between the two rotameters that means there is always enough oxygen delivered when the nitrous is in use.
Oh and by the way - they used to have CO2 rotameters to help encourage the patient to breathe at the end of surgery - I know right?
Our TikTok videos about rotameters
@anaestheasier Describe the features of a rotameter
♬ Round Round - Sugababes
@anaestheasier Replying to @maverick22066 ♬ original sound - Anaestheasier
Syllabus
- PC_BK_30 Measurement of volume and flow in gases and liquids, including pneumotachograph and other respirometers
Useful Tweets and Resources

Yup. The anaesthetic machine had a CO2 rotameter.
— bob funnekotter (@bobfunn) March 6, 2023
We gave just a whiff, I promise 🙏🏻
Also useful at the end of a case to kick-start spontaneous breathing 😀 pic.twitter.com/rSqODPwLOO
References and Further Reading

Primary FRCA Toolkit
Members receive 60% discount off the FRCA Primary Toolkit. If you have previously purchased a toolkit at full price, please email anaestheasier@gmail.com for a retrospective discount.

Discount is applied as 6 months free membership - please don't hesitate to email Anaestheasier@gmail.com if you have any questions!
Just a quick reminder that all information posted on Anaestheasier.com is for educational purposes only, and it does not constitute medical or clinical advice.