Actually understanding TCI
I found as a core trainee I was using TCI with increasing confidence, and starting to spot patterns in when it would work well and when I would need to start and stop the remi vs the propofol.
But I wasn't particularly happy with my actual understanding of what the pumps were doing, what the numbers meant, and what we were actually targeting when we tapped the patient's details into the pumps.
(We've written an exam-focused post on TCI and TIVA with the key bits you need to know on exam day, which we've linked at the bottom of this post.)
But today's post is a little different.
This post is Will's attempt to actually comprehend what happens when we hit that green button.
Come with me while I try to understand this properly.
Start simple and build
Please don't interpret the following few paragraphs as condescension, or an assumption that you don't already know a fair bit about how propofol and TIVA work.
It's just how my brain works.
I have to start at an incredibly basic level in order to understand it myself, and then I can build from there.
A single slug of propofol
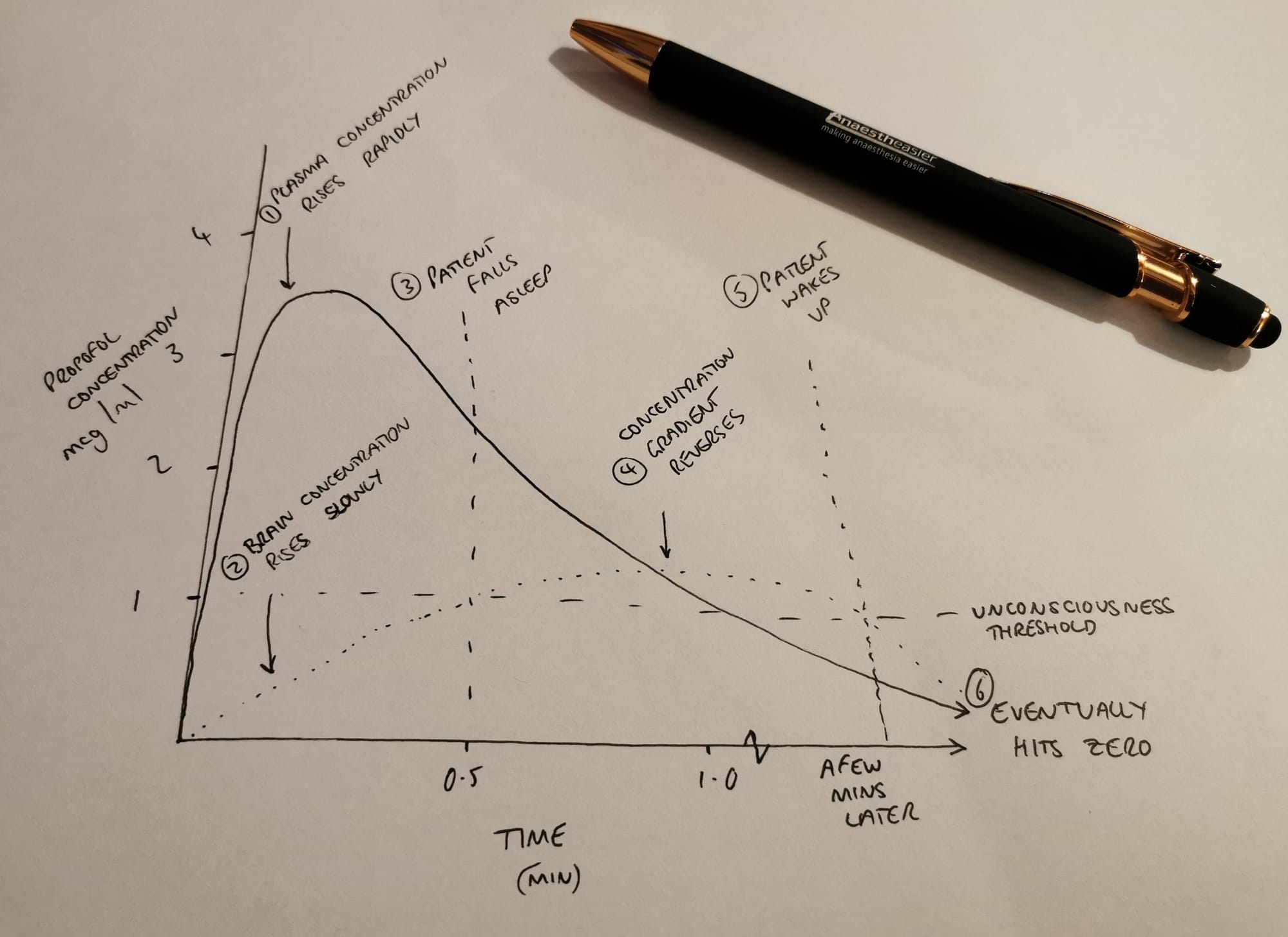
The simplest form of totally intravenous anaesthesia (TIVA) is a syringe of propofol given as a bolus, for example on a cardioversion list, or for sedation in the emergency department.
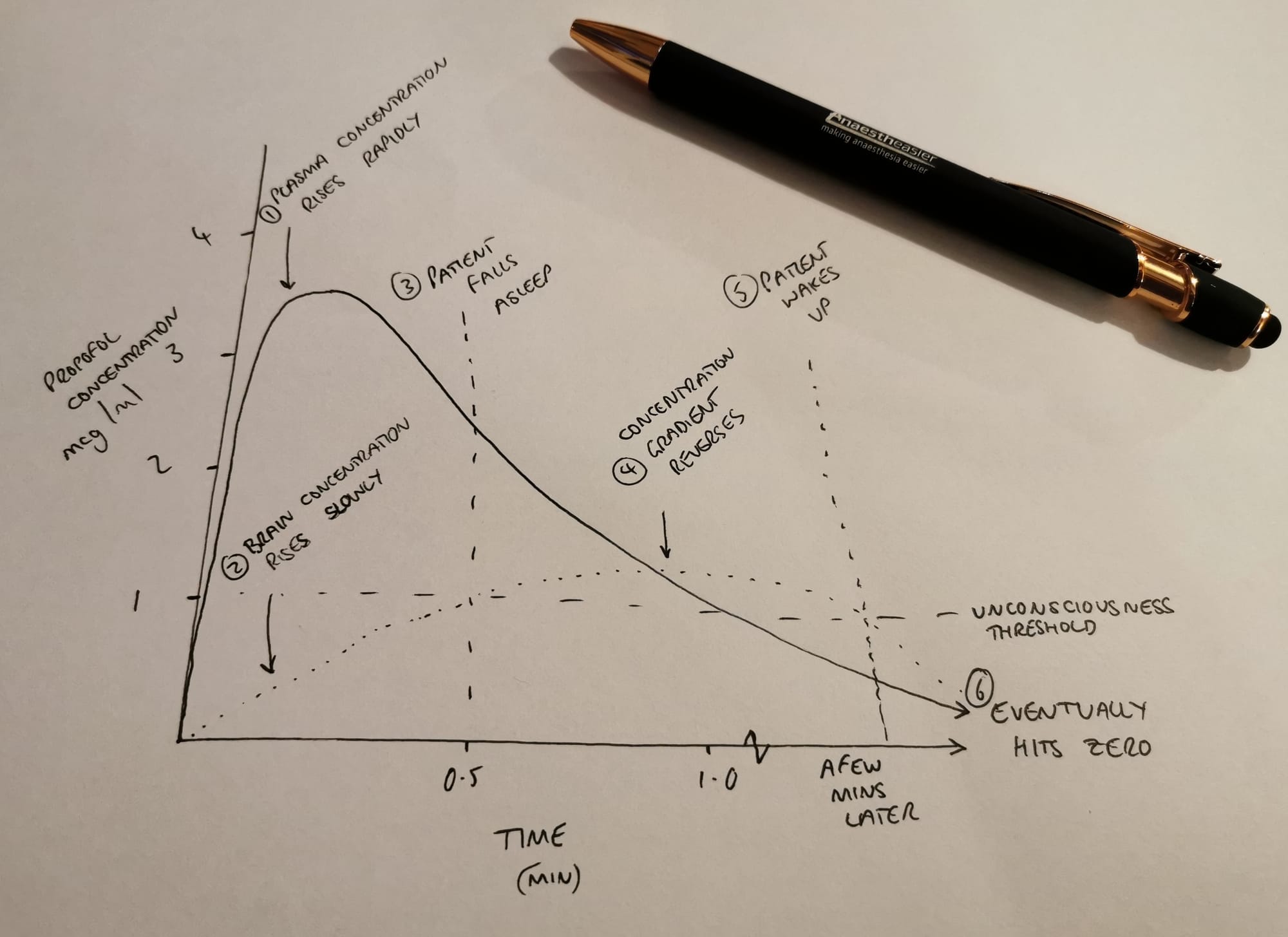
- Propofol enters the blood
- Plasma concentration rises rapidly
- Propofol-laden plasma is washed to the brain in around fifteen to thirty seconds depending on cardiac output
- A concentration gradient is established between plasma and brain
- Propofol diffuses into brain tissue (faster with a bigger dose and thus a bigger concentration gradient)
- When the plasma concentration reaches around 2 - 2.5 mcg/ml (ish) then the patient falls unconscious
- Propofol then rapidly redistributes from the plasma to other fatty areas in the body
- The plasma concentration drops exponentially
- The concentration gradient between plasma and brain tissue reverses
- Propofol diffuses out of the brain
- When the concentration drops below the unconsciousness threshold, the patient wakes up (usually after around five minutes, depending on the original dose)
- Most of the propofol is still inside their body but the concentration in their brain isn't enough to keep them asleep
- Eventually they metabolise and excrete the remaining molecules
Simple enough so far, but things change dramatically when you start talking about infusions.
Infusion time
Let's now entertain the idea you've managed to get your hands on an infusion pump. Not a posh one, but one that will give a ml/h infusion of your choosing, so you plumb in a big syringe full of propofol and hit go.
- Propofol enters the blood
- The plasma concentration of propofol starts to rise depending on the rate of infusion
Imagine these two situations
For the sake of illustration, let's picture two completely unreasonable scenarios:
- One where the infusion rate is set to the pump's maximum of 1200 ml/h
- One where the infusion rate is 0.0001 ml/h
Scenario 1
In the first scenario, the enormous rate of infusion will cause a huge spike in plasma concentration, a massive concentration gradient to the brain, and rapid, profound unconsciousness along with all the other side effects we try to avoid in our job.
Then as the infusion continues, the plasma concentration will continue to climb as the rate of infusion exceeds the rate of redistribution as well as the rate at which the liver and kidneys can eliminate it from the body.
The plasma concentration goes up and up, dragging the brain concentration and risk of a lawsuit with it.
Scenario 2
Now the infusion rate is pitifully low, meaning the propofol injected into the plasma is diluted so quickly by the venous blood that the concentration never reaches a clinically effective level.
The vast majority of the propofol molecules redistribute away from the plasma before doing anything helpful, and the liver and kidneys are able to clear the drug from the plasma faster than you're infusing it.
Some of the propofol still reaches the brain, but the concentration gradient is barely enough to encourage any molecules into the white matter, and the patient remains awake wondering how you got hold of a medical degree.
Clearly there is a sweet spot infusion rate somewhere between these two.
Now we have an issue to contend with.
When we gave a big bolus dose for our cardioversion, we spiked the plasma propofol concentration nice and high very quickly, which rapidly established an effective concentration gradient between blood and brain, allowing the patient to fall asleep in around thirty seconds.
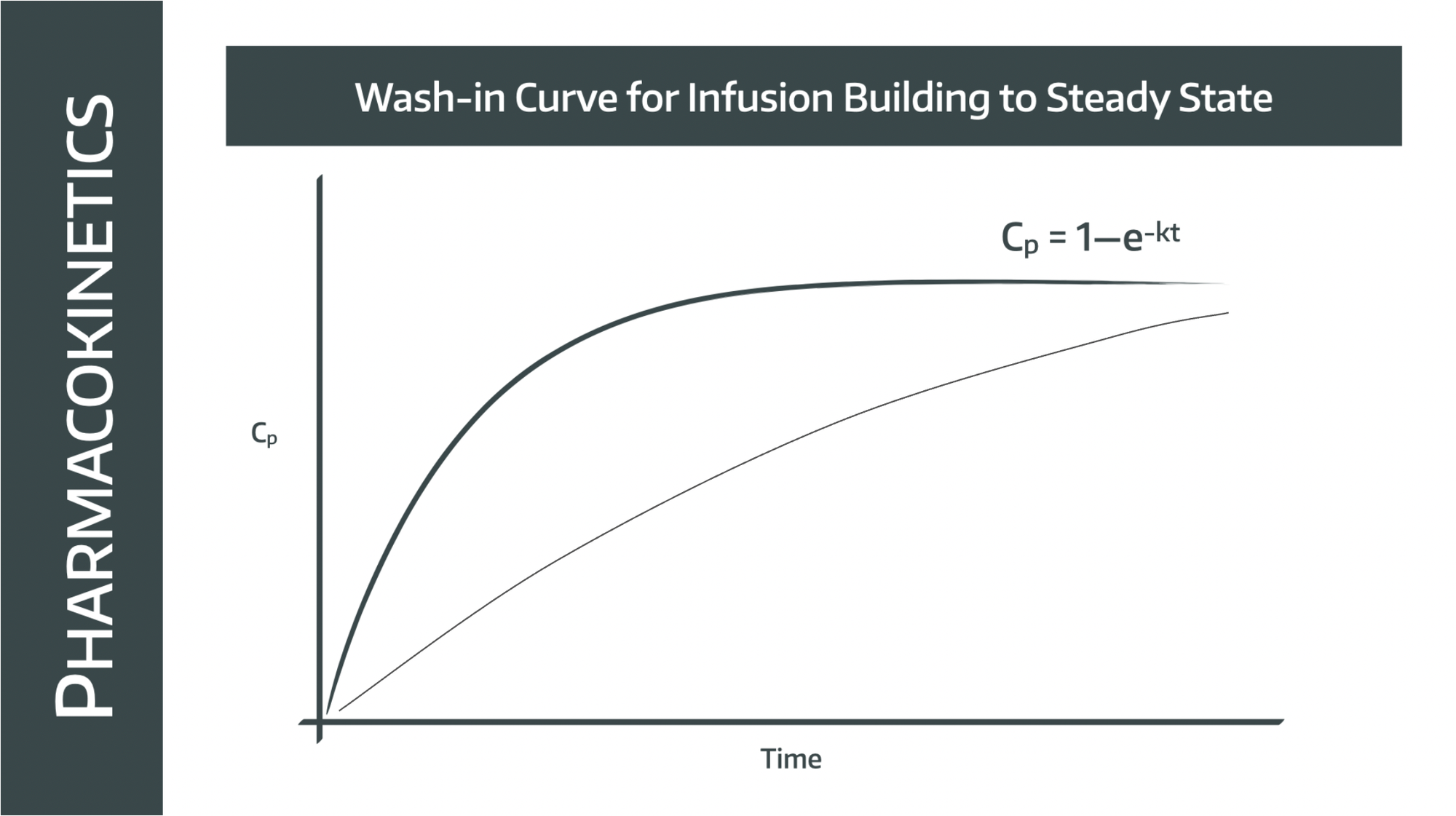
If we just set an infusion, however, the plasma concentration does this:
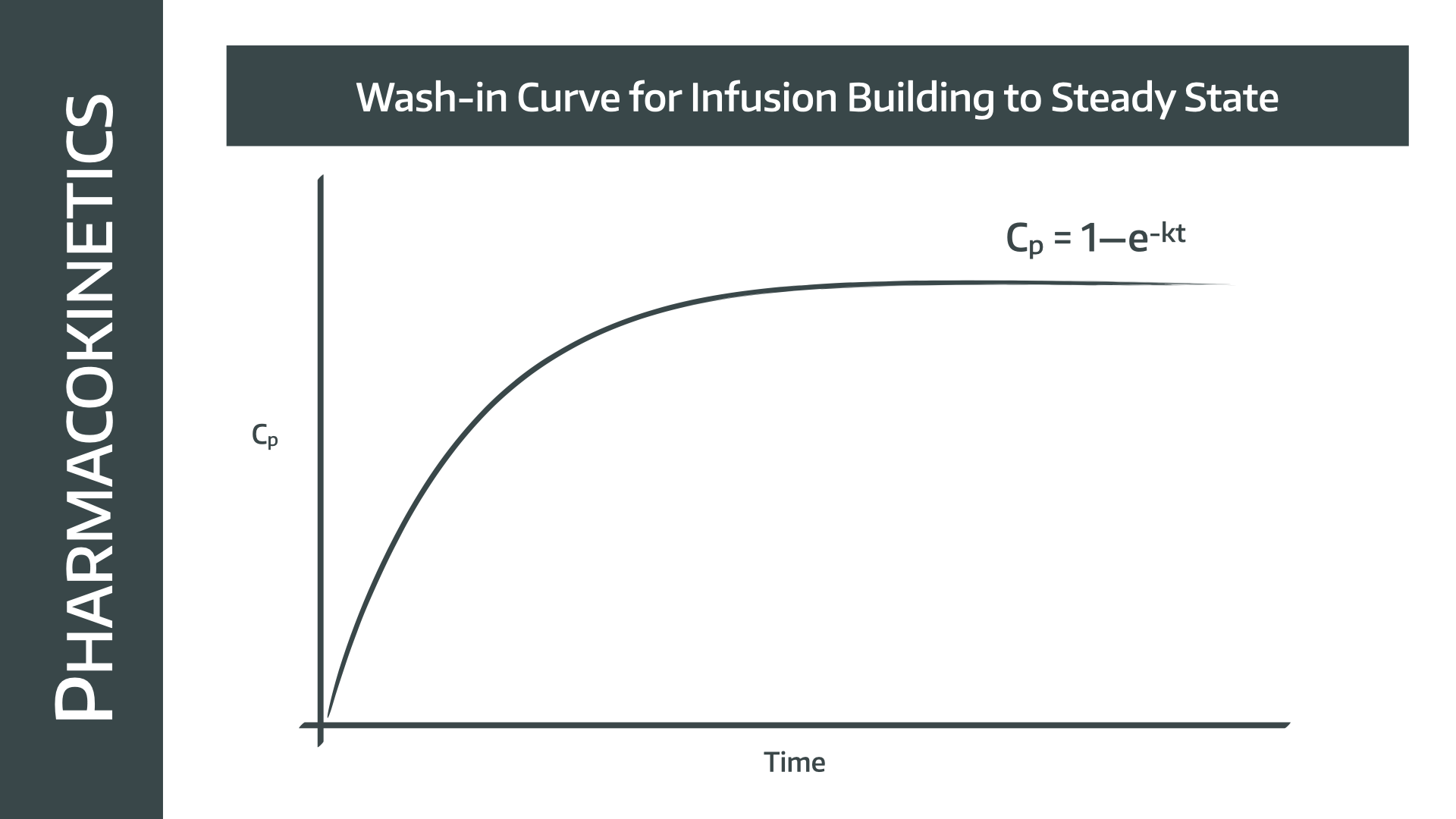
Remember the 'removal' from plasma includes redistribution as well as metabolism and excretion.
Eventually we'll get to a therapeutic plasma (and therefore brain) concentration, but it's not going to be a particularly efficient list.
So the simple solution to speed things up a little is to give a bolus injection as well, just to jump the plasma concentration up a little more rapidly and get the whole process rolling sooner.
Simple enough so far - bolus to get to sleep quickly, infusion to keep them there.
When the bucket fills up
So here we get more complicated quite quickly, because the redistribution phase starts to become more relevant.
Let's say we've given a bolus and are now steadily infusing propofol to our sleeping patient.
- Some diffuses into the brain
- Some distributes into fat and other tissues
- Some gets metabolised and excreted
If these three were all happening at constant rates, we could just match them with a set ml/h infusion and be done with the whole thing, safe in the knowledge that our patient is asleep and we're not heading towards dangerously high levels of plasma propofol.
But life just isn't that simple.
The rate at which propofol redistributes from the plasma into the tissues is initially rapid, as there is an enormous concentration gradient between plasma and fat, however as the operation draws on the fatty compartments of the body start to fill up with propofol, and that concentration gradient begins to flatten.
And the rate of redistribution drops.
Eventually (like, after 20 hours) all of the body's fat will be pretty saturated with propofol, and there will be no further redistribution.
What factors impact the redistribution phase?
Thinking logically, if you're pouring propofol into what is essentially a massive storage bucket of fat, then this process is going to be affected by:
- How much propofol you're using
- How fast you're pouring it
- How big the bucket is
- How quickly it's leaking out
This is why TIVA pumps care about age, height, weight and gender, because all of these impact how big the fat reserve (bucket) is, and thus how extensive and rapid the redistribution and elimination processes are going to be.
The TIVA pump will use these parameters (depending on the model) when calculating how much it will need to infuse to compensate for redistribution, and for how long.
There will of course still be metabolism and excretion of propofol, but for the most part when looking at normal-length operations, this pales in significance to the redistribution process.
What are compartments?
To make a sensible guess at how much propofol to give and how fast, we need to know where the molecules are going and how quickly.
We need a model.
These 'compartments' are the representations in our model of the different areas of the body that the propofol can end up in, including:
- Blood
- Brain
- Liver
- Muscle
- Fat
- Other organs
- Skin
You get the idea.
Now when trying to model how propofol is going to behave, you could try and work out how much propofol is going to end up in every single different compartment in the futile pursuit of perfect accuracy.
This would require knowledge of exact blood flows, fat content and diffusion constants into every possible anatomical space.
Clearly this is entirely infeasible.
Alternatively you could lump all of the compartments into one and just treat the body as a single homogeneous fluid cavity throughout which the propofol evenly distributes itself.
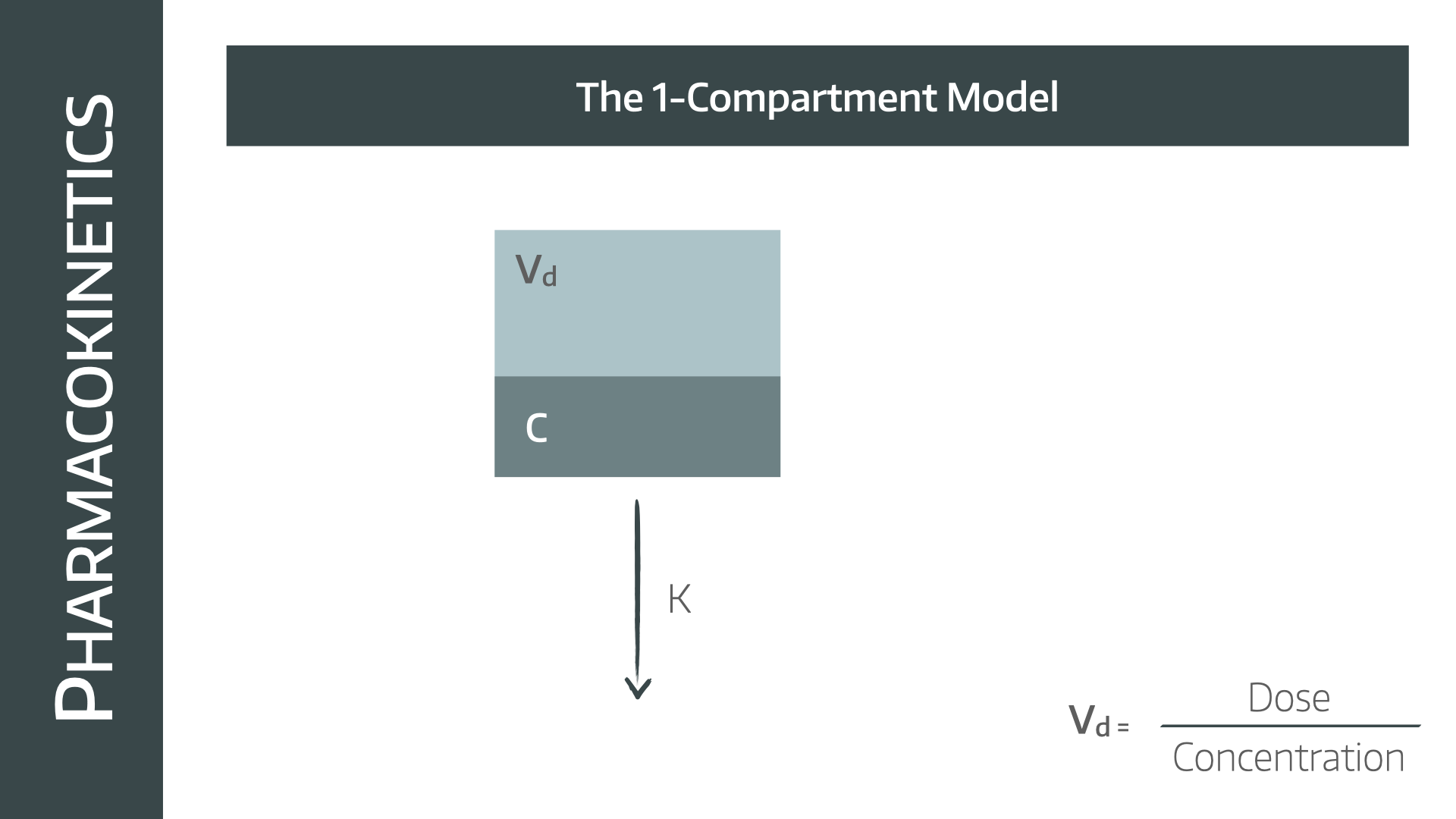
This is the one compartment model which assumes:
- You infuse propofol into the body
- It evenly distributes throughout the whole body
- The measured plasma concentration would therefore be the same as the concentration in every organ including the brain
- The propofol is eliminated by the liver and kidneys at some rate K
Hopefully by now it's reasonably obvious why this is not going to give us an accurate representation of how propofol molecules are actually going to behave, because it doesn't explain the 'redistribution' phase that we've already discussed.
What if we add another compartment?
Okay let's now split the model into two:
- Blood (some texts also include the heart, liver and kidneys here)
- Everything else (including brain, muscle, fat and other organs)
We can still only add and remove propofol from the body via the central compartment which is the blood or V1.
The liver and kidneys are still doing their job removing the molecules at some rate K, except since it's now not the only rate constant to think about, we have to label it K10 (because it's from compartment 1 to outside the body).
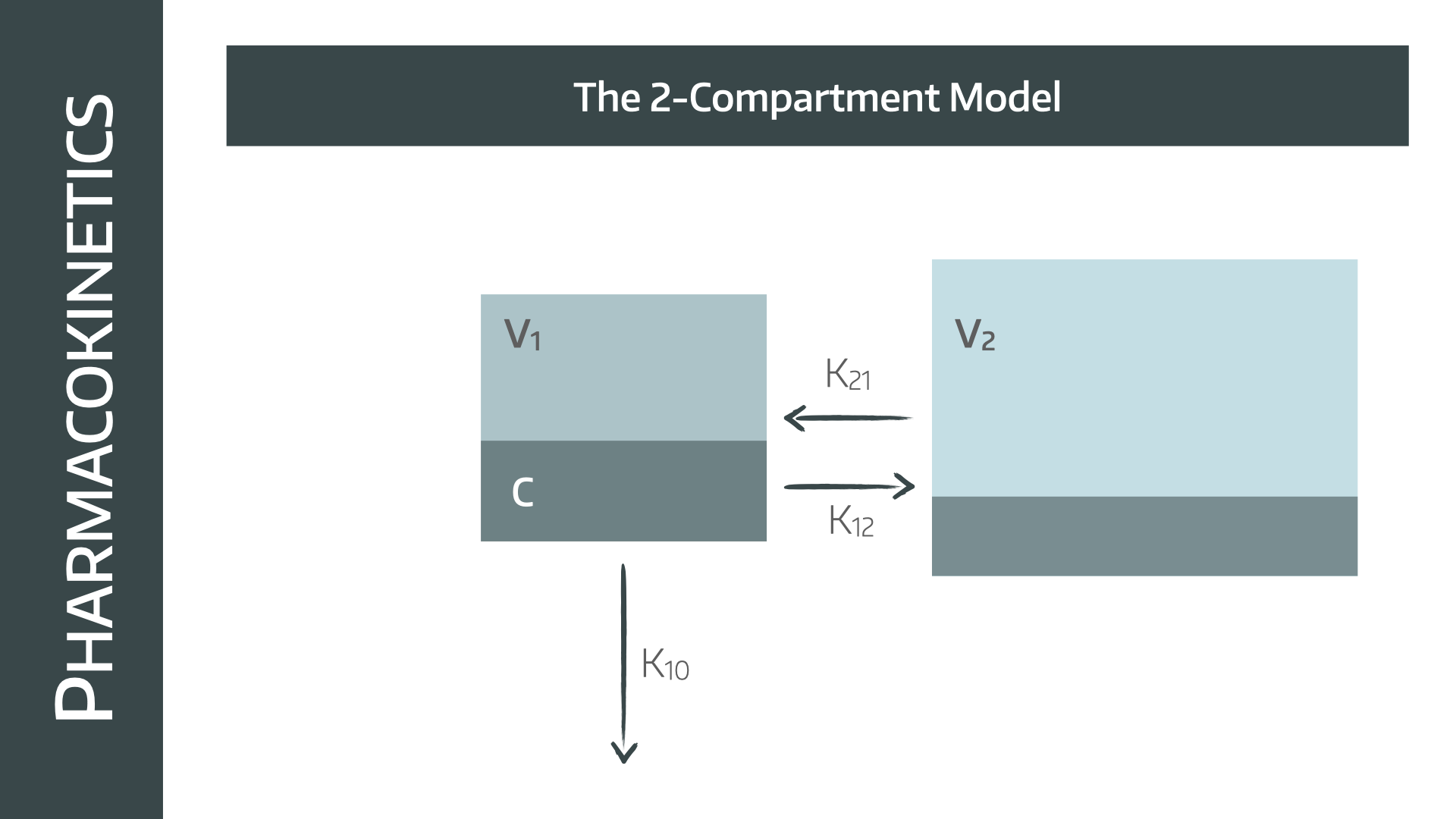
This allows us to explain the redistribution concept a little better, because we now have a second rate constant between V1 and V2 that is going to depend on the concentration gradient between the plasma and the everything else compartment.
- Propofol is shoved into V1
- The concentration of V1 increases
- A concentration gradient between V1 and V2 is established
- Propofol diffuses into V2
- This process continues until the gradient is flat and the concentrations are equal
- Propofol is removed from V1 by the liver and kidneys
- The concentration gradient reverses between V1 and V2
- Propofol diffuses back out of the everything else compartment
- Eventually it's all cleared from the blood
Seems to make sense.
So why don't we use this model?
Because it still doesn't work when you try and use it, because the plasma concentrations predicted by the model don't quite align with the measured concentrations when you test it on real people.
So let's chuck in another compartment and see what happens.
The three compartment model
Now we're talking.
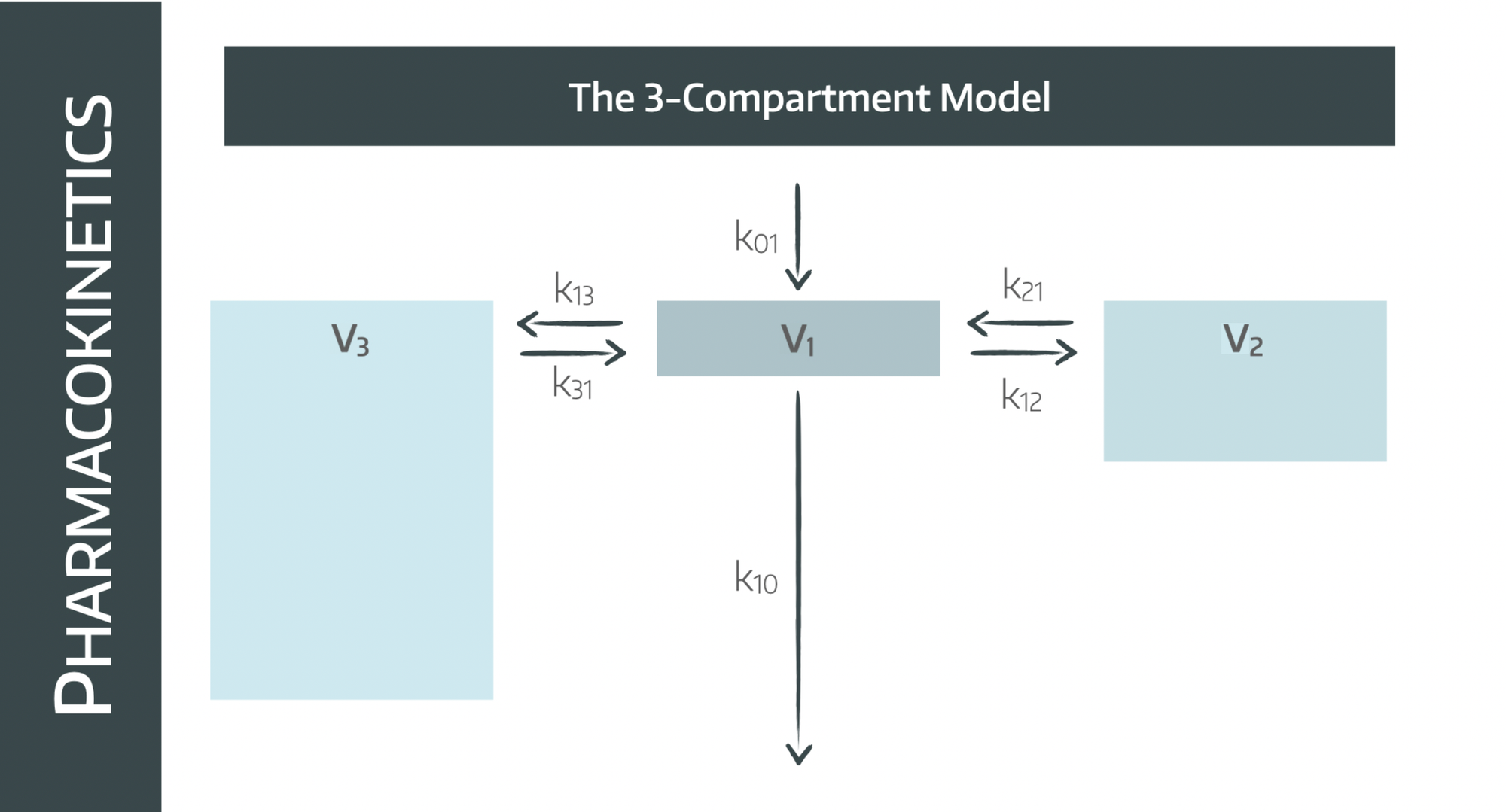
Not much has actually changed here, all we've done is split V2 into V2 and V3.
Note that they are of different sizes.
- V1 = central compartment = blood (and heart and liver etc if you want)
- V2 = rapid distribution compartment = brain and muscle
- V3 = slow distribution compartment = fat and other bits and bobs
This model is better because it acknowledges the fact that some organs have much larger blood supplies than others, and therefore the rate of propofol redistribution is going to differ.
The brain and liver concentrations of propofol rise much more rapidly than that of the subcutaneous fat, because the perfusion is so much better.
However the volume of poorly perfused fat is enormous compared to the highly perfused organs, and this is reflected in the model as demonstrated above.
The other processes are exactly the same:
- You can only add (Ko1) or remove (K10) from the central compartment
- Propofol will distribute down concentration gradients
- The gradients will reverse once the infusion stops and the propofol starts to be eliminated
What's nice about this model is it fairly accurately predicts the observed plasma concentrations.
Look at the graph below and you see the plasma concentration dropping in an exponential fashion after a bolus dose of propofol as is expected when rate of elimination from the plasma is dependent on concentration.
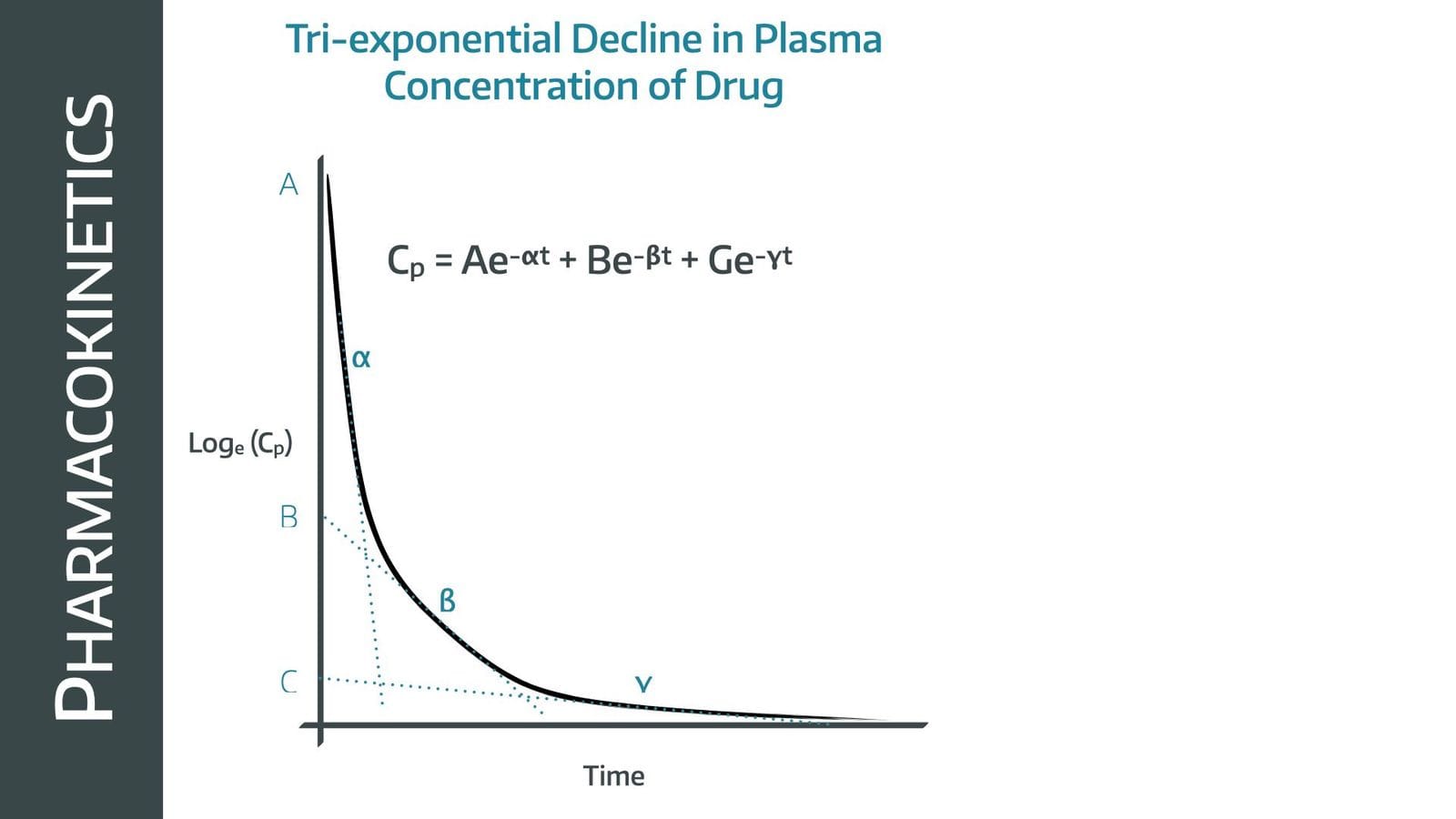
But what's really cool is this graph isn't a perfect single exponential but the product of three seperate processes, representing the propofol diffusing back out of V2 and V3 into the plasma, effectively 'autotransfusing' the plasma and keeping the plasma concentrations slightly higher as these reservoirs drain.
Shall we add another compartment?
You could, and it might make the algorithm slightly more accurate, but at the expense of enormous complexity with diminishing returns.
Don't let the pursuit of 'perfect' stop you from enjoying 'good enough'.
Most TCI models are quite content with three compartments.
Right, so what is 'effect site'?
Great, so the effect site is the unimaginative name for the place where the drug is actually having a clinical impact.
The following nuance is very important.
The effect site is in the brain, but it is not just 'the brain', because once the propofol is delivered to the cerebral circulation it still has to:
- Diffuse out of the plasma across the blood brain barrier
- Diffuse into the myelin
- Diffuse into the lipid bilayer of the neuron's membrane
- Find the GABA-A receptors
- Attach itself to the correct binding site
- Induce a conformational change
- Wait for a molecule of GABA to bind
- Hold the channel open long enough for sufficient chloride to hyperpolarise the neuron
- Continue this process until enough neurons in the network required to maintain consciousness are sufficiently hyperpolarised to prevent meaningful conscious experience to manifest
So yah, takes a little time.
This is why we can say that the brain itself is in V2, because it has a rich blood supply and the propofol distribution to the organ is rapid, but the effect site is not.
When we talk about effect site concentration, we're simply talking about the plasma concentration + a bit more maths to explain what's taking so long.
Repeat: while the effect site is anatomically situated inside the brain, for the purposes of our model, it is an entirely separate mathematical concept.
And that is why the final diagram looks like this:
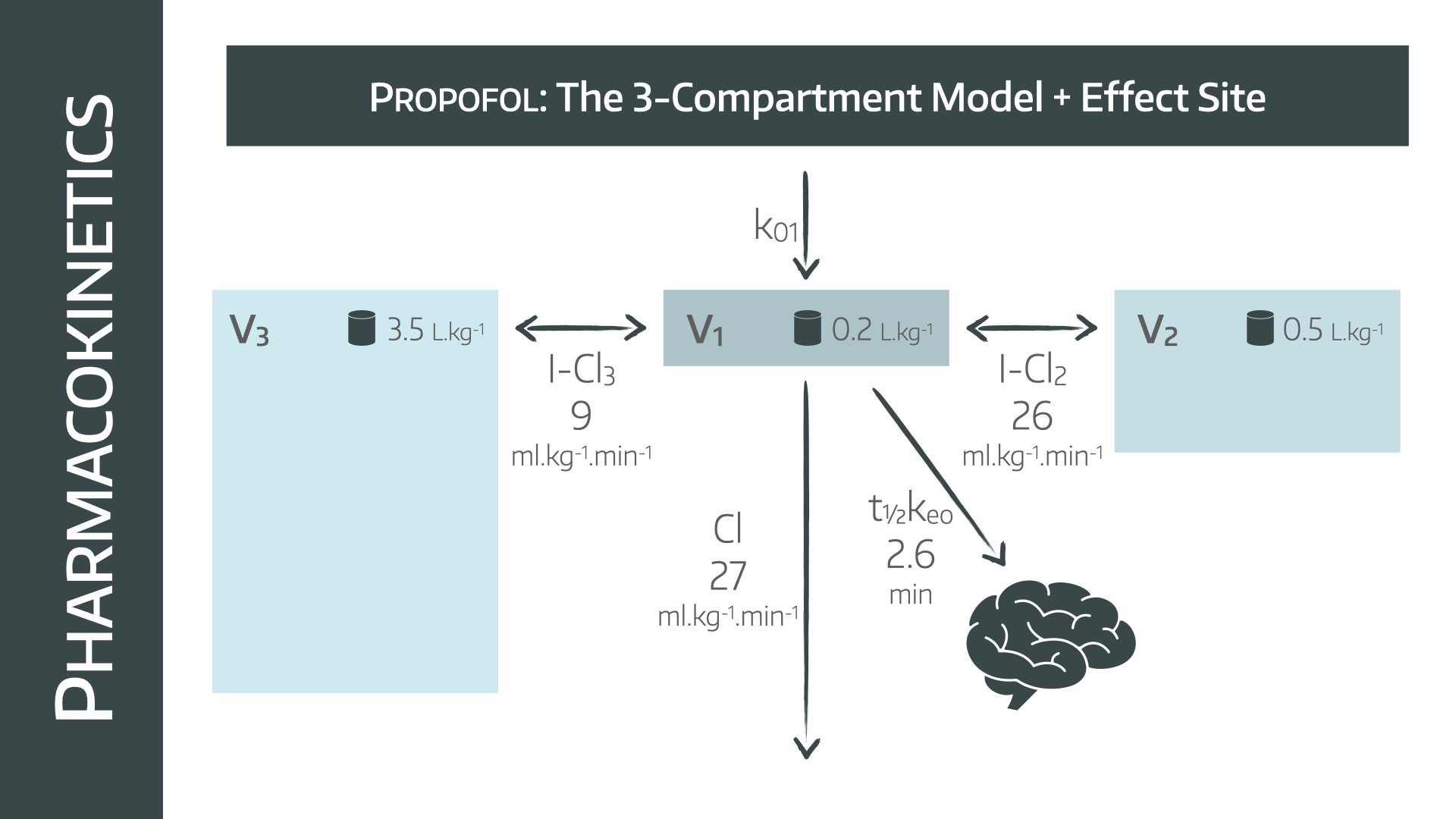
This is why the rate constant that is used to explain the changing effect site concentration is Ke0, and not just K12, which merely models the physical concentration of propofol in the brain tissue.
Enter the models
Now we finally talk about the TCI models that we actually use in day to day clinical practice.
- Marsh
- Schnider
- Eleveld
Hopefully these names aren't entirely new by now.
But what does it actually mean when you say your pump is 'using' the 'Marsh' or 'Eleveld' model?
It means that your pump is doing a whole bunch of really cool maths every ten seconds to predict what the current plasma and effect site concentrations are, and then adjust the rate of infusion in order to achieve whatever target you've told it to.
This maths is designed to:
- Estimate how big the patient’s available total 'propofol space' is
- Estimate how quickly propofol moves between compartments (K12, K21, K13, K31)
- Estimate how quickly the body clears it from the blood (K10)
- Estimate how fast the brain equilibrates with plasma (Ke0)
It therefore has an algorithm (the model) that tells it:
- The volume of V1
- The volume of V2
- The volume of V3
- The rate of drug clearance from the plasma
- The rate of Ke0
- The rates of K12 and 21, and K13 and 31
Then you come along and plug in whatever details it asks for (height, age, weight, sex etc) and it then adjusts the above values depending on how the algorithm tells it to use those parameters.
- Marsh adjusts the three volumes with total body weight but leaves the rate constants untouched and ignores the patient's age
- Schnider keeps V1 at a fixed volume of 4.7 litres, keeps V3 and its rate constant fixed, but then adjusts V2 and its rate constants, and the elimination rate constant depending on age, weight and lean body mass
As a result, they behave very differently, because the difference between how the models handle the estimated volume of V1 is insane.
- Schnider says everyone has a V1 of 4.7 litres
- Marsh meanwhile says that V1 is around 0.228 L/kg × weight
- So an 85 kg man has a V1 of 19.4 litres
- And a 140 kg man has a V1 of 32 litres
So now it makes total sense why Marsh gives a much larger initial bolus dose than Schnider, because to achieve the same plasma concentration, even in a slim individual, it thinks its working with four times the volume!
It also shows why Marsh tends to overdose obese patients, especially elderly, as it ignores age and blindly assumes requirements increase fairly linearly with total body weight, which we know not to be true.
All hail Eleveld
This is the new kid on the block, and I'm incredibly biased, but it’s hard not to be impressed by Eleveld.
- It was tested on more patients
- It was tested on a much wider age range
- It dynamically changes a whole host of parameters based on age, weight, sex, lean body mass, maturation and whether other drugs such as opioids are in use
This is lifted from the original paper, which is linked below:
- 15 433 propofol concentration and 28 639 BIS observations from 1033 individuals (672 males and 361 females) were analysed
- The age range was from 27 weeks postmenstrual age to 88 years
- The weight range was 0.68-160 kg
- The final model uses age, PMA, weight, height, sex, and presence/absence of concomitant anaesthetic drugs as covariates
A 35-yr-old, 170 cm, 70 kg male (without concomitant anaesthetic drugs) has a
- V1 of 6.28 litres
- V2 of 25.5 litres
- V3 of 273 litres
- CL of 1.79 litres min-1
- Q2 of 1.75 litres min-1
- Q3, of 1.11 litres min-1
- ke0 of 0.146 min-1
And it just works.
Okay so what is the 'target'?
This is what the pump is aiming for.
Are you telling it to achieve and maintain a set plasma concentration (Marsh) or a set effect site concentration (Schnider and Eleveld)?
Once you're at steady state infusion six hours into some maxillofacial horrendoplasty the difference is going to be minimal as the compartments reach near-equilibrium, however for induction it makes a massive difference.
Look at these two images again:
When we gave a bolus dose, the plasma concentration shot up, and the effect site concentration followed fairly swiftly, but when you just target a plasma concentration the effect site takes a while to catch up.
A pump that is targeting effect site concentration knows that this will lag behind the plasma concentration depending on what it thinks the rate of Ke0 is.
Schnider's V1 is so small that if you try and use it to target plasma concentration it will give an insufficient bolus dose and you risk under-anaesthetising your patient.
To get around this issue, Schnider targets effect site concentration, rather than plasma concentration, and hugely overshoots the calculated plasma concentration in the process.
This is how the Schnider gets away with such a small V1, proving that size doesn't matter, it's about how you use it.
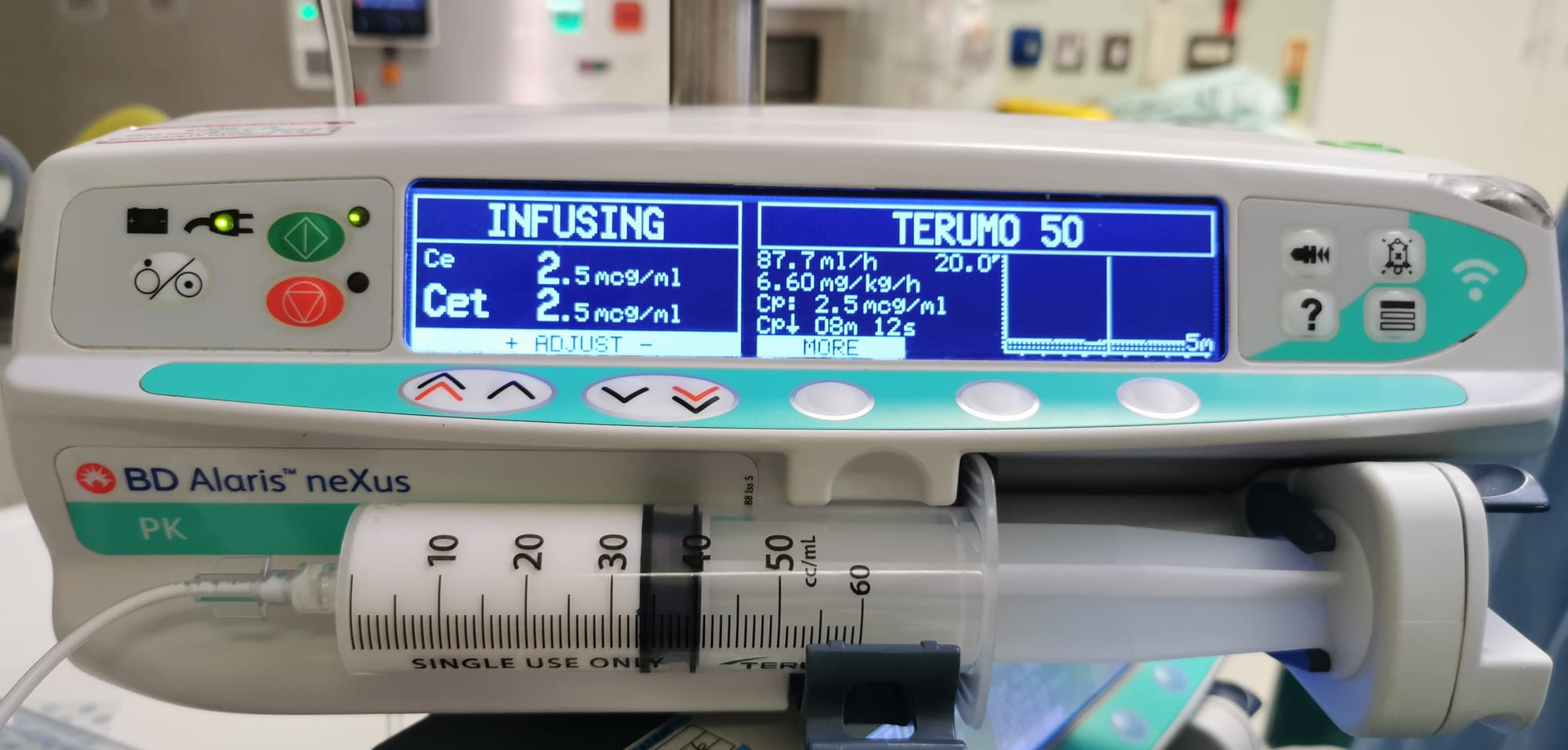
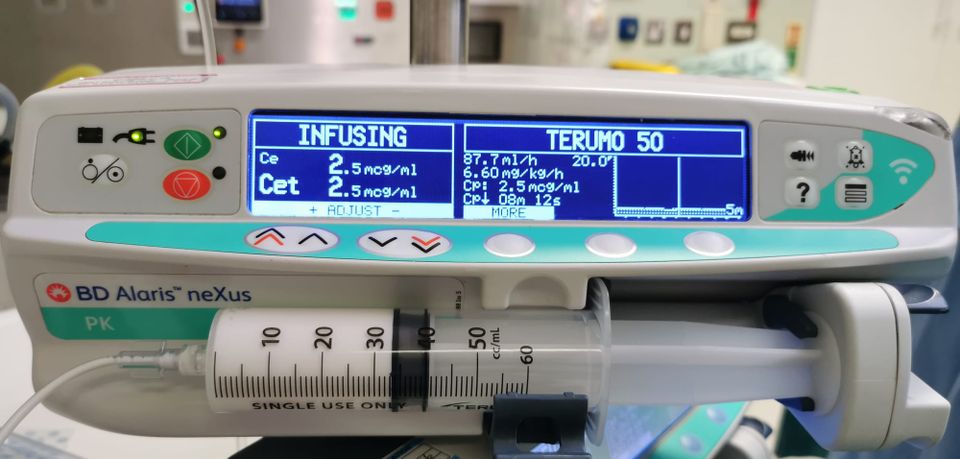
Here you can see the Eleveld model targeting an effect site concentration of 2.5 mcg/ml.
- Cet is the target it's aiming for
- Ce is what it thinks it currently is
- You can also see Cp on the right, which logically is at the same level
- It also tells you that to achieve this it is currently infusing at 6.6 mg/kg/h or 87.7 ml/h
- This infusion rate will be completely different at different stages of the anaesthetic, as the pump is continually calculating and readjusting based on all the parameters we have discussed (while also taking into account how much propofol it has already given, at what rate, and for how long)
IT'S SO INSANELY COOL
I'm done now.
Wake up time
Switch the infusion off and we stop giving any new propofol to the patient.
- The plasma concentration drops (redistribution, metabolism and excretion)
- The concentration gradient between plasma and brain now swings in favour of propofol leaving the brain
- The brain (effect site) concentration drops
- Once the concentration drops below the unconsciousness threshold, the patient wakes up
The eagle-eyed reader will immediately rebut with 'I thought the redistribution had stopped because all of the fat had filled up?'
And you're absolutely right, depending on the length of operation.
- After a single bolus of propofol, the plasma concentration drops very rapidly as redistribution has only just begun, and the metabolism and excretion component is essentially irrelevant
- After a three-day infusion of propofol on intensive care, the plasma concentration drops far more slowly, as the fat is saturated with propofol and there's not much capacity left for redistribution
This is called context sensitive half time and it refers to the idea that the duration of a drug's clinical effects will depend on how long you have been infusing the drug for.
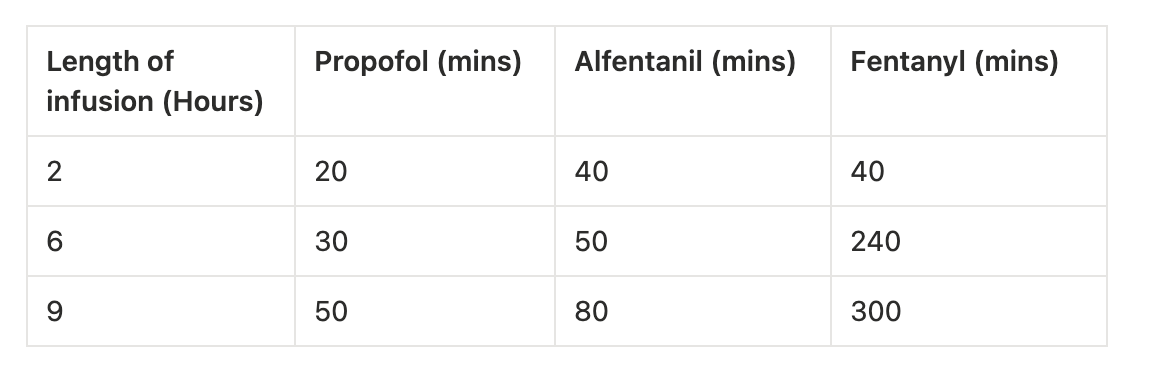
Compare this to remifentanil, where the insanely rapid breakdown of the opioid means it doesn't matter how long you've been infusing it for, it's going to wear off in less than ten minutes every time.
Which is in part why many anaesthetists like high-remi, lower-propofol TIVA regimes for long cases, because the patient wakes up much faster.
This is what the little Cp with the down arrow means in the picture:
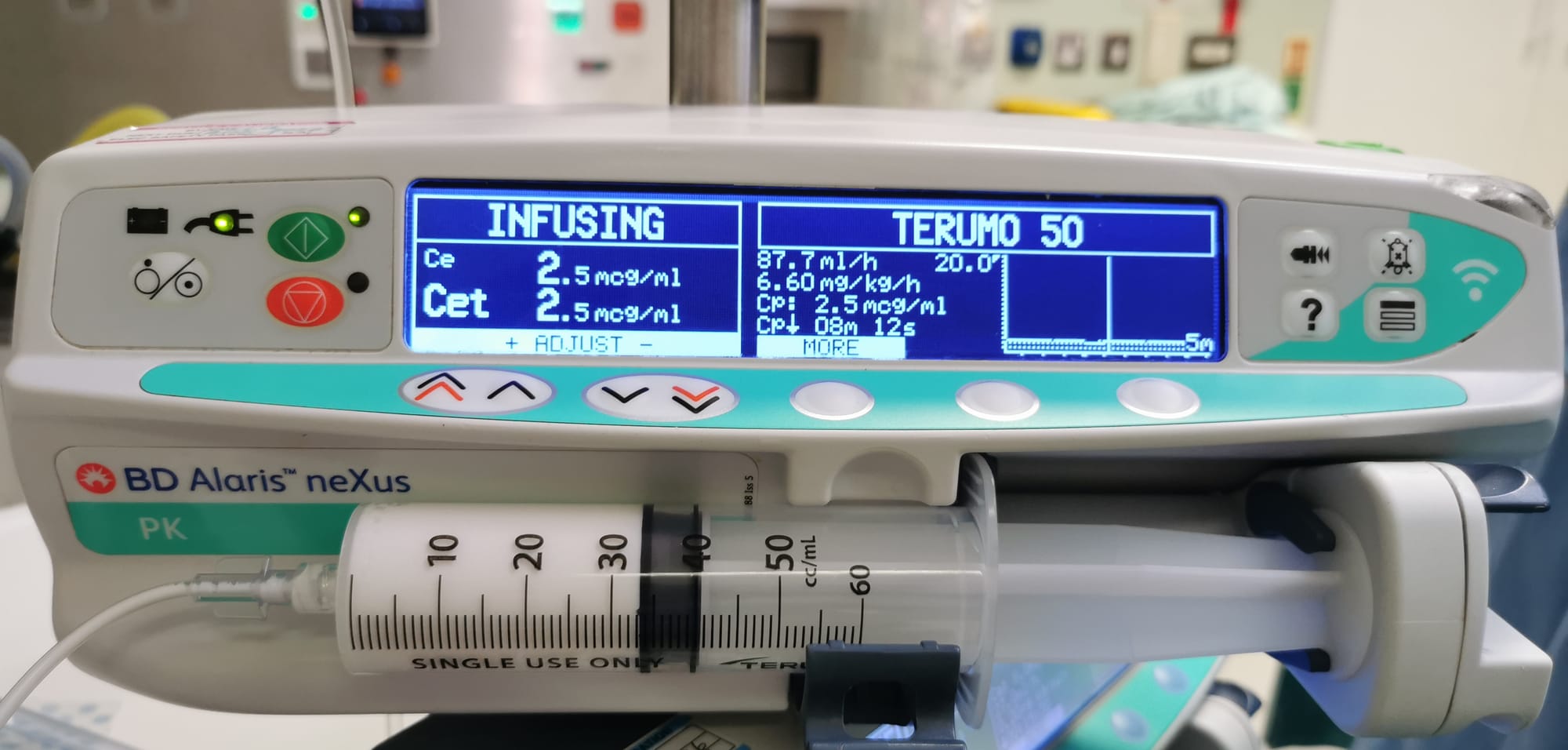
It's saying 'If you stop the infusion now, it's going to take around 8 minutes for the plasma concentration to drop to the point where I think this patient will wake up'.
Noice.
Very long story short
We want to give the patient enough propofol to ensure they're nicely asleep, but not so much that we delay wake up or cause unnecessary side effects.
So in order of increasing 'scientific-ness' (and defensibility) our options are:
- Push the plunger on the syringe and stop when the patient closes their eyes, then give them little top ups every so often based on heart rate and blood pressure
- Calculate a mg/kg initial dose, and run a ml/hour infusion, again titrated to heart rate and blood pressure
- Use a manual TIVA infusion model such as the Bristol model
- Use a target controlled infusion (TCI) pump that takes a patient's height, weight, age and gender (and for Eleveld, whether you're using opioids as well) and then predicts the patient's blood and brain concentrations at any given time, adjusting the infusion rates as necessary to keep it at a target level, ideally titrated to BIS or other processed EEG waveform*
- Do the same but with AI monitoring the patient's monitoring and real-time propofol plasma concentration and autonomously adjusting infusion rates to optimise comfort, list efficiency, cost, environmental impact based on the patient's medical history and test results, and the surgeon's historical operating behaviour**
*Note that it doesn't know what the actual plasma or brain concentration is, because it's not measuring anything. It's exceptionally accurate guesswork based on a very complicated and a fairly robustly validated algorithm.
**Not currently available in my trust.
Get in touch
Hopefully at least some of this was even remotely helpful for clarifying TCI a little.
Not a word of this was written by AI.
It is entirely the work of a caffeine-addled middle grade registrar who is crucially, a massive nerd who really enjoys tapping away on his computer. Therefore there are potentially some errors, for which I can only apologise.
If anything I've said doesn't make sense, or is incorrect, please don't hesitate to ping us an email at anaestheasier@gmail.com so we can figure it out together.
Some of our videos
Here's our exam-focused post

References and Further Reading