Traumatic Diaphragmatic Hernia

The Case
A 47 year old man presents to the ED with acute onset left sided chest pain, shortness of breath and vomiting after a few days of generalised upper abdominal discomfort.
Last month he was involved in a significant road traffic collision however was not found to have any major injuries and was sent home with analgesia.
This delay can be a long time, we're talking years potentially.
On examination he is:
- Tachycardic
- Mildly hypoxic
- Significantly distressed
You listen to his chest as part of his primary survey, and you find reduced air entry over the left hemithorax, and you think you can hear bowel sounds instead.
The chest xray looks like this:

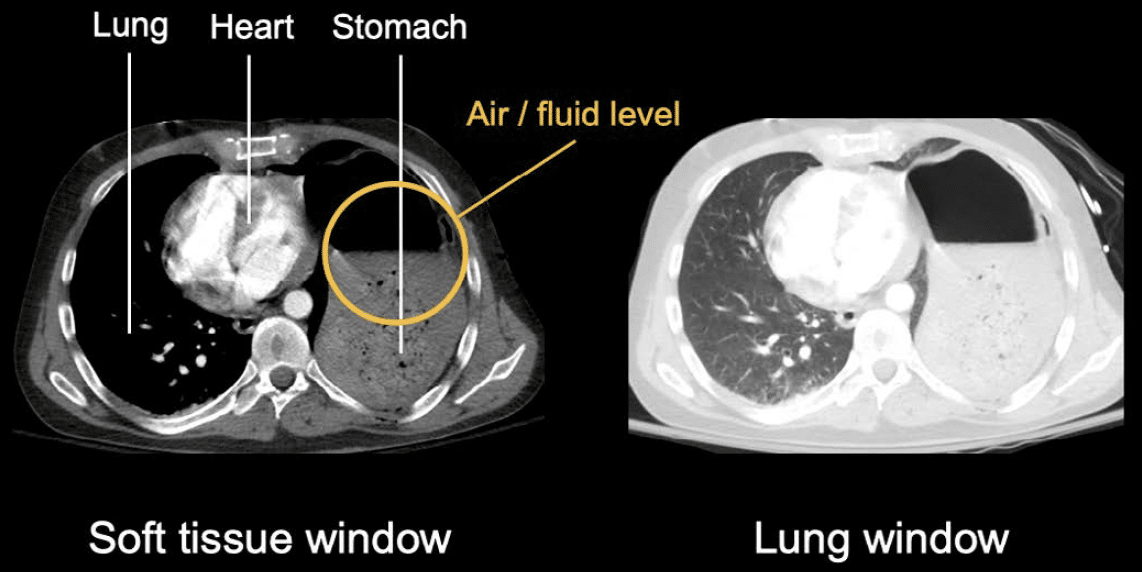
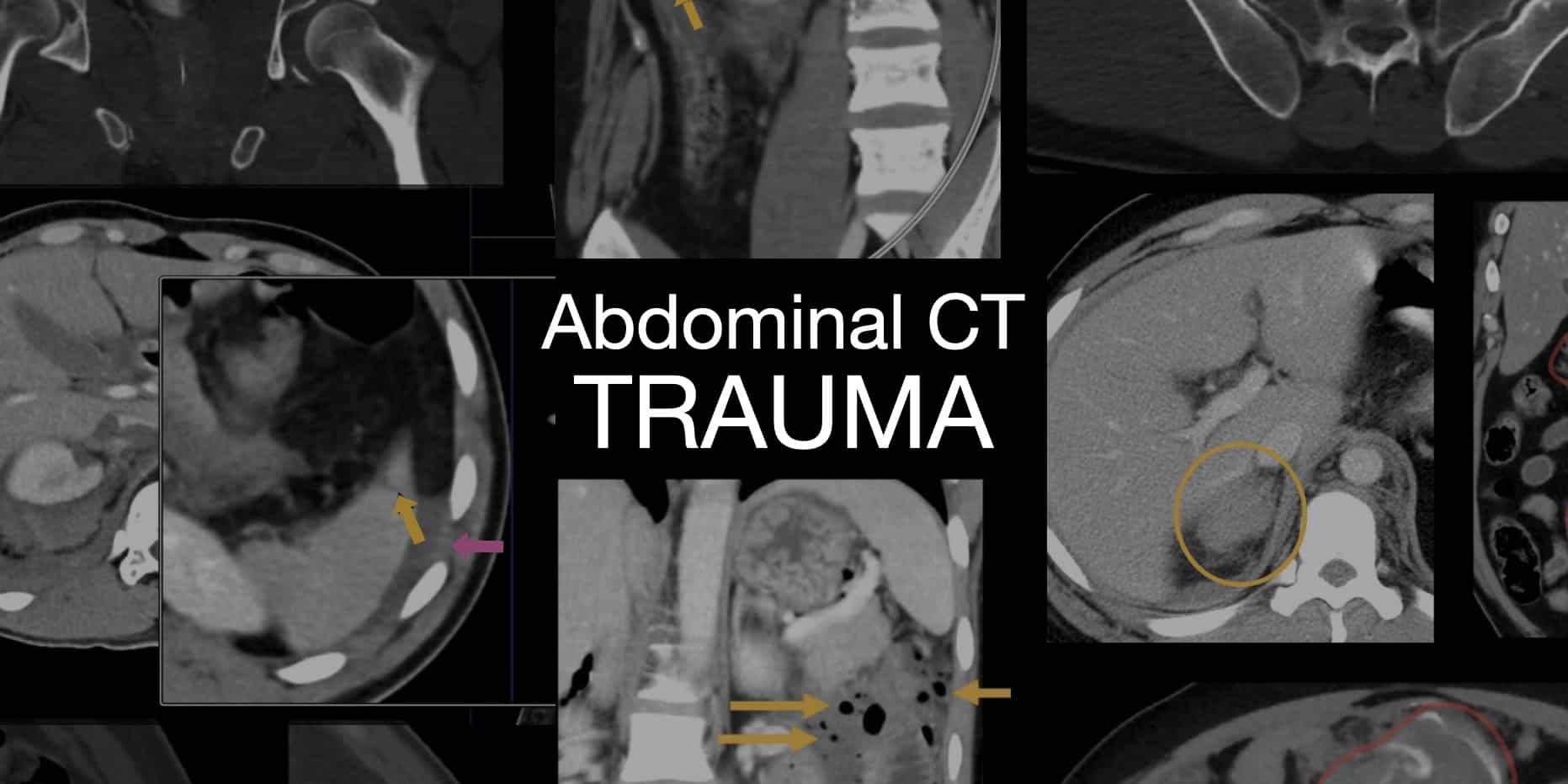
And the CT scan looks like this.
"How on earth did they miss this last month?" I hear you cry.
Because it didn't look like that last month.
These injuries are frequently missed during the initial trauma assessment because the diaphragmatic defect may be small, chest radiographs can be normal, and more obvious injuries often dominate the clinical picture.
While the trauma to the diaphragm occurs acutely, it can take time for the herniation to occur, and even longer for it to start causing problems for the patient.
Why this gets examined
- Resuscitation and trauma management
- Emergency thoracic and abdominal surgery
- Airway management with aspiration risk
- Complex respiratory mechanics
- Potentially catastrophic haemodynamic compromise
- Double lumen tubes
- Postoperative pain management
What are the common causes of traumatic diaphragmatic injury?
- High speed road traffic collisions
- Penetrating thoracic or abdominal trauma
- Falls from significant height
- Crush injuries
How might this patient present?
Usually they're asking this to see if you can appreciate the difference between acute and delayed presentations of this condition.
Acute
- Polytrauma or major trauma patient
- Respiratory distress
- Chest and abdominal pain
- Haemodynamic instability
- Hypoxia
Delayed
- Reduced exercise tolerance
- Recurrent aspiration or chest infections
- Dyspnoea
- Bowel obstruction
- Acute abdomen
- Sepsis from strangulated bowel
Pathophysiology
The physiological consequences depend on the size of the defect caused by the traumatic event, and of course which organs are involved.
What exactly happens?
- Sudden increase in transdiaphragmatic pressure gradient
- Radial tear of diaphragm
- Progressive enlargement over time (hence the delayed presentation)
- Negative intrathoracic pressure gradually pulls abdominal organs into chest
- Usually it's stomach, colon or small bowel
- It's more common on the left because the liver provides some protection to the right side
Although using your liver as a crumple zone to protect your diaphragm seems slightly counterproductive.
Respiratory
- Hypoxia
- V/Q mismatch - enormous shunt in area of compressed lung
- Restrictive respiratory deficit
- Reduced FRC
Standard stuff you'd expect from the lung having an unwanted gastric room mate.
Cardiovascular
- Reduced venous return
- Reduced cardiac output
- Mediastinal shift
- Direct cardiac compression
In severe cases the haemodynamic compromise can mimic that of a tension pneumothorax.
Gastrointestinal
- Vomiting
- Bowel obstruction
- Gastric volvulus
- Strangulation
Clearly this patient is going to be high risk for aspiration.
So what's the plan?
The first and most obvious point to make is this patient needs emergency surgery to fix their traumatic diaphragmatic hernia.
Which means they're also going to need:
- Primary survey to assess for even more urgent injuries
- Resuscitation and haemodynamic stabilisation
- Rapid sequence induction
- Thorough multimodal pain control
- Close monitoring on critical care afterwards
What are your key concerns for anaesthetising this patient?
This is an acutely unwell patient presenting for emergency surgery, with:
- Respiratory and haemodynamic compromise
- High risk of aspiration
- Potential bowel obstruction
- Other possibly life threatening injuries
As always, when asked in the final FRCA exam, 'how would you anaesthetise this patient?', you're going to break your answer down thusly:
- Preoperative
- History and examination
- Investigations and imaging
- Resuscitation and optimisation
- Intraoperative
- Induction and airway management
- Maintenance and intraoperative care
- Emergence
- Postoperative
- Discharge destination
- Analgesia and antiemetic plan
History and examination
On top of a full anaesthetic history and examination, you want to pay particular attention to:
- Other injuries including c-spine
- Oxygen requirement
- Evidence of respiratory compromise
- Evidence of haemodynamic compromise
- Exercise tolerance
- Comorbidities
Is there anything else that's going to make this even trickier?
Investigations and imaging
- Bloods - bleeding, infection
- CXR - stomach in chest, mediastinal shift, lung volume reduction
- CT - identification of abdominal organs in thorax, evidence of ischaemia and obstruction
- ECG - and echocardiogram if significant haemodynamic compromise
Resuscitation and optimisation
- Large bore IV access and fluid resuscitation
- Analgesia
- Antiemetics
- NG tube - to empty stomach and improve respiratory mechanics
- Crossmatch and blood if bleeding
Induction
- Monitoring - full AoA monitoring, arterial line, consider CVC if unstable
- Positioning and preoxygenation - head up, consider HFNO
- Rapid sequence induction and endotracheal intubation
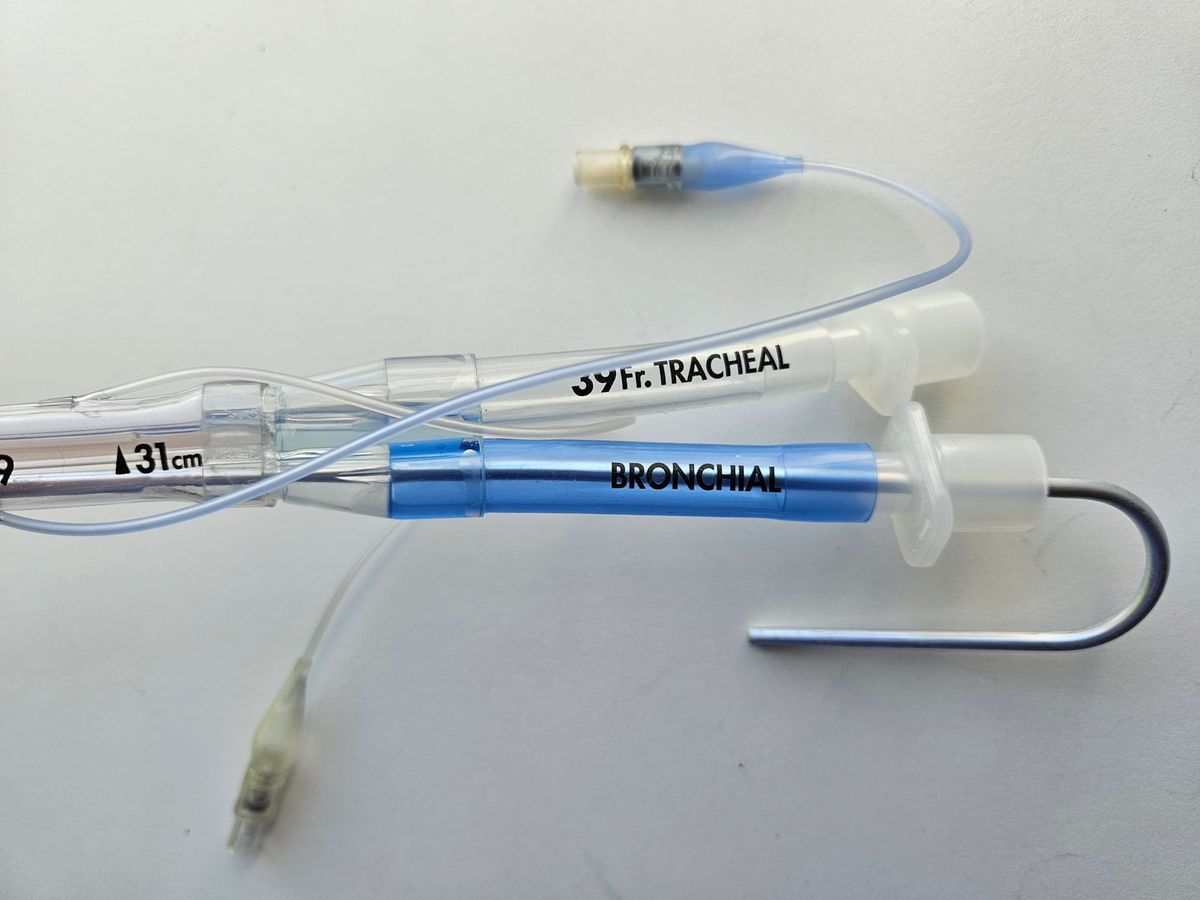
- Double lumen tube or bronchial blocker if one lung ventilation required*
*Not all repairs require lung isolation, it will depend on the surgical approach (laparotomy, thoracotomy, thoracoscopy).
The examiner may then dive off down the rabbit hole of double lumen tubes, which we've covered in this post.
Why might this patient become unstable after induction?
- Loss of sympathetic tone
- Reduced preload due to intrathoracic compression and hypovolaemia*
- Hypovolaemia due to vomiting, poor intake and bleeding
*Made worse by positive pressure ventilation.
Maintenance and intraoperative care
As always, gas or TIVA depending on your institution and what is safer in your hands.
- Expect high airway pressures and reduced lung compliance
- Oxygenation may be difficult if significant shunt
- Lung protective ventilation is usually a good idea
- Catheter to monitor urine output
- Close temperature and blood glucose control
- Replacement of blood products where necessary
It's a good idea to explicitly mention that you'd avoid excessive airway pressures and PEEP in a patient with raised intrathoracic pressure.
The patient suddenly becomes hypotensive intraoperatively, what are your thoughts?
This could be multifactorial, and you need to address each in turn:
- Reduced venous return
- Tension physiology
- Bleeding
- Septic shower
- Vagal stimulation from pleura or peritoneum - especially if suddenly bradycardic
How would you manage hypoxaemia during one lung ventilation?
The key here is this is most likely due to shunt, so just increasing the FiO2 probably isn't going to achieve a whole lot.
- Increase FiO2
- Call for skilled assistance
- Check the tube position
- PEEP to dependent lung
- Consider CPAP to non-dependent lung
Why might the airway pressures suddenly jump intraoperatively?
- Viscera are returned to the abdominal cavity
- Abdominal pressure increases
- Reduced diaphragmatic excursion
- Reduced compliance
- Increased airway pressure
How are you going to extubate this patient?
You first need to decide whether they're safe to extubate.
- Ongoing shunt and high oxygen requirement
- Ongoing respiratory compromise from diaphragmatic splinting
- Cardiovascular instability
There may be many reasons to keep them asleep on intensive care for a while.
If you do decide to extubate, aspirate the NG tube and do it the same way you would for an emergency bowel obstruction laparotomy - wide awake.
Postoperative care
- Destination is usually HDU or ICU after major emergency thoracic surgery - may require ongoing ventilatory support*
- Analgesia - multimodal, opioid sparing, epidural may be appropriate
- Antiemetics - multimodal and generous
*Need to watch out for re-expansion pulmonary oedema as well as postoperative ileus and sepsis from strangulated bowel.
What are your options for postoperative regional anaesthesia?
- Thoracic epidural
- Paravertebral block
- Erector spinae plane block
- Serratus anterior plane block
- Intercostal block
- Interpleural block
Key take home message
References and Further Reading


Other related posts


Just a quick reminder that all information posted on Anaestheasier.com is for educational purposes only aimed at trained professionals, and it does not constitute medical or clinical advice.
Anaestheasier should not be used as a definitive resource for academic writing, please reference original source material.
Anaestheasier® is a registered trademark.