Preoxygenation

What is it?
Preoxygenation, or denitrogenation, is the process of washing the predominantly nitrogenous room air out of a patient's lungs and replacing it with wholesome organic* pure 100% oxygen.
*unverified.
In clinical practice this looks like popping on your anaesthetic facemask with a seal to prevent the patient from entraining any room air, and instructing the patient to do one of two things:
- Normal breathing for three minutes
- Eight full vital capacity breaths
Either is fine, but what you're looking for on the monitor is the end tidal oxygen concentration to be as high as possible, ideally above 90%.
But why do we bother?
It's simple maths
Let's say you are anaesthetising that mythical 75 kg Mr Average patient we read about in the textbooks, breathing room air (21 kPa of oxygen) at sea level, and you receive a dose of muscle relaxant.
- You stop breathing
- Your chest wall muscles relax
- Your thoracic volume decreases to functional residual capacity (by definition)
How long until you're dangerously hypoxic?
Well let's assume for argument and easy maths sake that your FRC is around 2.5 litres.
Now let's remember from the alveolar gas equation that by the time room air reaches the alveoli, you're down to a partial pressure of around 13 kPa.
- 2.5 litres of 13% oxygen = 325 ml reservoir of oxygen in your lungs
- Normal oxygen consumption under anaesthesia is approximately 250 ml/min
- This means you have around 1 minute and 20 seconds to get that tube in
After this your PaO2 is going to start to drop rather precipitously.
Now let's preoxygenate
This time you've sensibly preoxygenated Mr Not-so-average for three minutes or eight full vital capacity breaths, and have nicely denitrogenated your lungs, and have an end tidal oxygen concentration of around 90%.
- 2.5 litres of 90% oxygen = 2250 ml reservoir of oxygen at FRC
- Assuming you're still consuming 250 ml/minute
- This means you now have a reserve of around 9 minutes
That's a lot more time that you can spend faffing around in the pharynx before your patient is going to be in serious danger.
This is why we preoxygenate.
Much like the range of an electric car, in real life clinical practice safe apnoea time is significantly shorter than advertised, due to shunt, atelectasis and increased oxygen consumption.
What is the definition of safe apnoea time?
- Time from onset of apnoea to oxygen saturations of 90%
Who needs it most?
You can often predict who is going to desaturate quickly just by looking at them.
- High BMI
- Large neck
- Respiratory disease
- On oxygen already
- Floridly septic with high respiratory rate
All of these situations predispose to desaturation, be that because the airway has become occluded after induction, the FRC is collapsed down to the size of a teacup or the oxygen consumption chews through the reserve in a matter of seconds.
You might have noticed when this happens, that the sats hover around 98-99% and slowly start to dip, but as soon as you get below 95%, it all gets a lot worse very quickly.
This is because while the PaO2 will drop at a fairly steady pace, the SaO2 of haemoglobin will remain high thanks to its cooperative binding, until the oxygen tension is sufficiently low that each haemoglobin can no longer bind four oxygen molecules.
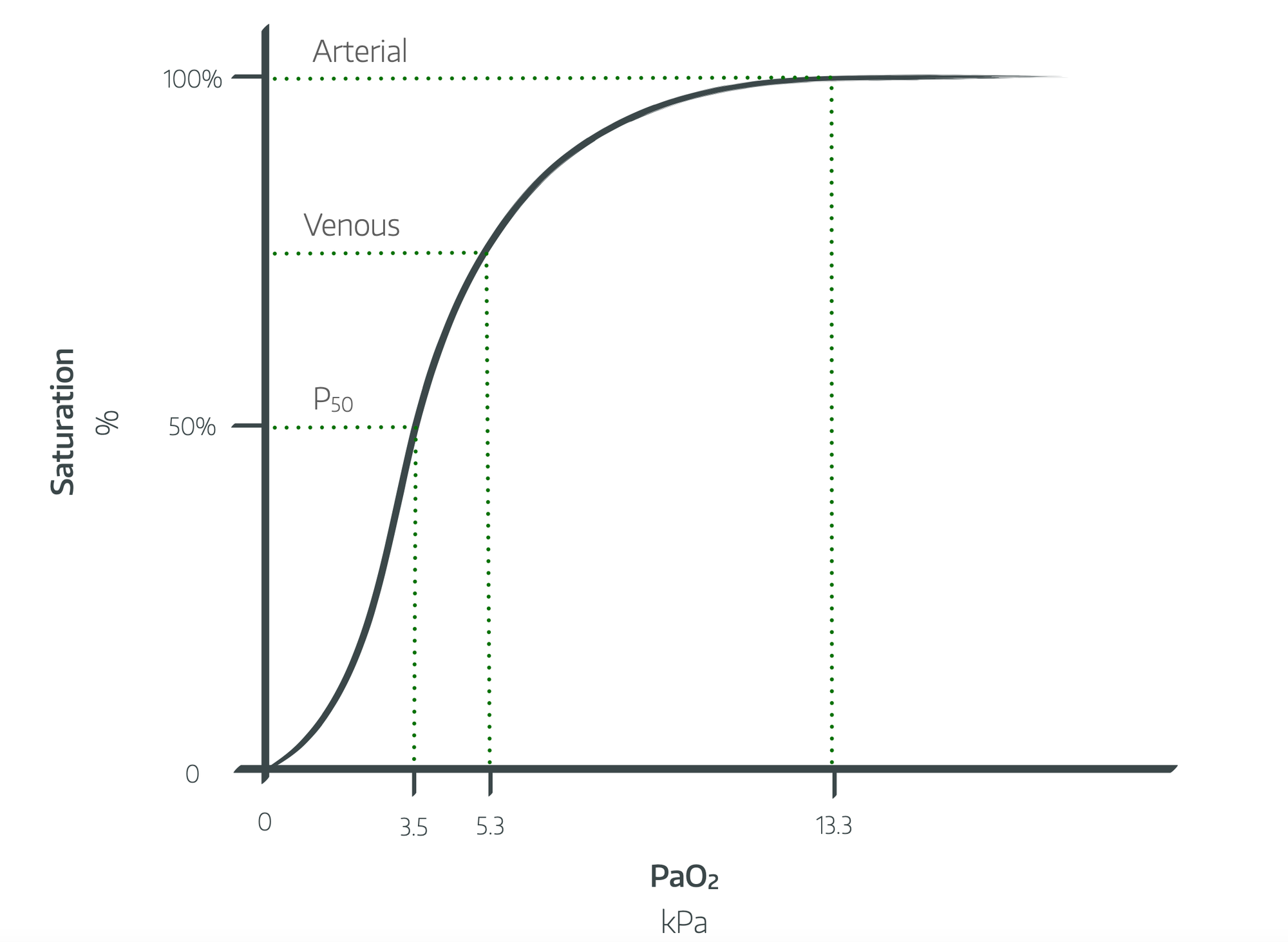
Once the sats start to drop below 90% (at a PaO2 of around 6 or 7 kPa), you can expect them to drop by around 30% per minute if you don't rectify the situation fairly promptly.
How do I prevent this?
By employing as many of the following techniques as you possibly can:
- Preoxygenate thoroughly to achieve an end tidal CO2 of at least 80%
- Do this in a head-up position ideally of at least 30°
- Use high flow nasal oxygen as well as your normal facemask
- As soon as the patient is asleep, pop in a supraglottic airway and ventilate them while you wait for the rocuronium to work
- Or slip an oropharyngeal airway in and facemask ventilate them
- At the very least use some PEEP to hold the airway open
If you're really not keen on ventilating them before intubating, you can hold their face in a strong jawthrust, applying peep with a facemask while the optiflow provides some apnoeic oxygenation.
Personally I'd choose the IGEL and ventilate option, because if it works well, you know that you can fall back to plan B safely if the intubation is more difficult than expected.
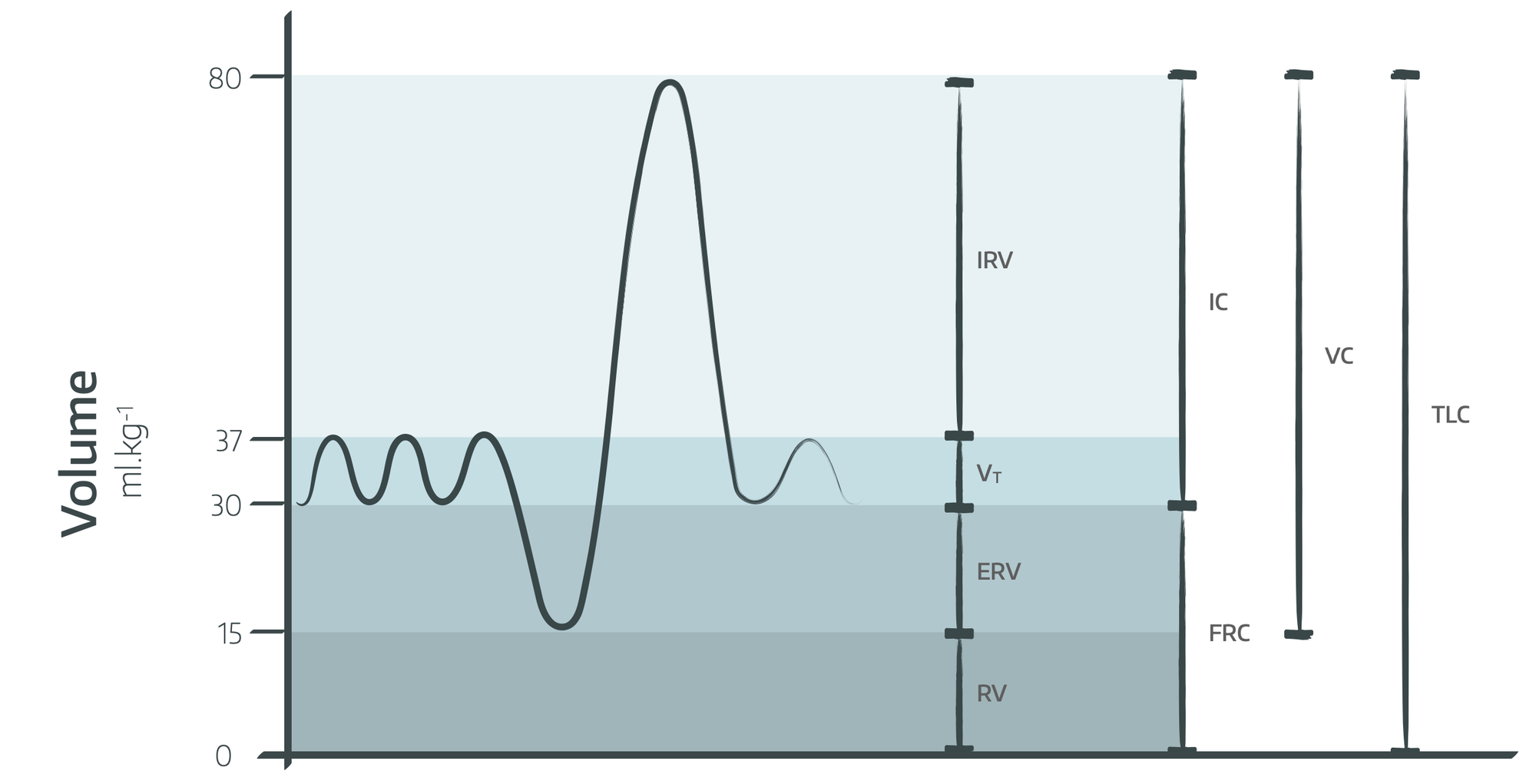
How does obesity affect preoxygenation?
- Decreased vital capacity
- Decreased expiratory reserve volume
- Decreased inspiratory capacity
- Decreased functional residual capacity, which decreases further in the supine position (to around 1.8 litres)
- More likely to have a difficult airway
- Increased oxygen consumption rate
Patients with obesity class III will desaturate three times faster than a patient with a normal BMI.
What about pregnancy?
Thankfully, data are rather limited when it comes to the question of 'how long does it take a pregnant woman to critically desaturate while apnoeic?'
- FRC is dramatically reduced by baby and abdominal organs pressing on diaphragm
- Supine position makes this even worse
- Rate of oxygen consumption is up to 30% higher at term
What about critical illness?
It shouldn't surprise you that critically unwell patients desaturate more rapidly, for a variety of reasons:
- Cardiac pathology
- Respiratory pathology
- Anaemia
- Hypermetabolism
- Poor cardiac output and perfusion
- VQ mismatch
- Airway obstruction
- Poor respiratory effort and pain
Preoxygenation will not provide you with the same degree of buffer, but is even more important in the critically unwell patient.
Not sure if you remember that pandemic we had a little while back...
What about kids?
Apnoeic kids desaturate up to three times faster than adults because of:
- Smaller FRC
- VQ mismatch
- Faster oxygen consumption
- Splinting of diaphragm by stomach
Same idea - preoxygenation is more difficult but also more valuable.
Why holding the airway open really matters
You've veritably 'boshed' your patient off to sleep and are patiently waiting for the timer to tick around to tell you the roc is cooked and the cords are ready for tubing.
Why hold the airway open?
Surely you've got this nice reservoir of oxygen in their chest, so why does a patent airway matter at this point?
Say hello to CO2
Right now you're probably consuming around 250 ml/min of oxygen and at the same time, your blood is dumping around 200 ml/min of CO2 into the alveoli.
This volume difference of 50 ml/min generates a slight negative pressure that draws more air in on the next breath, and is essentially clinically insignificant.
However.
In your anaesthetised and apnoeic patient, CO2 clearance from the alveoli stalls, and as a result the partial pressure gradient between pulmonary capillary and alveolus flattens.
Since CO2 is so soluble in water, it doesn't mind and just sits in the blood for a while. But as you're still consuming 250 ml/min of oxygen, this means that the volume in:volume out ratio enlarges dramatically, with much more gas being removed from the alveoli than returned.
This creates negative intrapulmonary pressure and contributes to airway collapse and hypoxia.
Unless the airway is patent.
If the airway is patent, then fresh gas can be drawn in to replace the lost volume, and if this replacement gas is 100% oxygen because you're dutifully clamping the facemask onto the patient's face, and holding their pharynx open with an adjunct, then happy days.
The end result is apnoeic mass transfer of oxygen into the lungs, which prolongs the safe apnoeic time prior to intubation dramatically.
Theoretically, in perfect lungs, this can maintain oxygen saturations for up to 100 minutes. However hypercapnia and acidosis become life-threatening well before this.
What factors will affect time to critical hypoxia?
- FiO2
- Patency of airway and apnoeic oxygen transfer
- Functional residual capacity
- Alveolar membrane function (lung disease)
- Anaemia
- Rate of oxygen consumption
Prepare for landing
You should also preoxygenate for extubation, or any time there might be some airway silliness where a patient will thank you for having had a reserve of oxygen to use while their vocal cords pulled themselves together (or apart again).
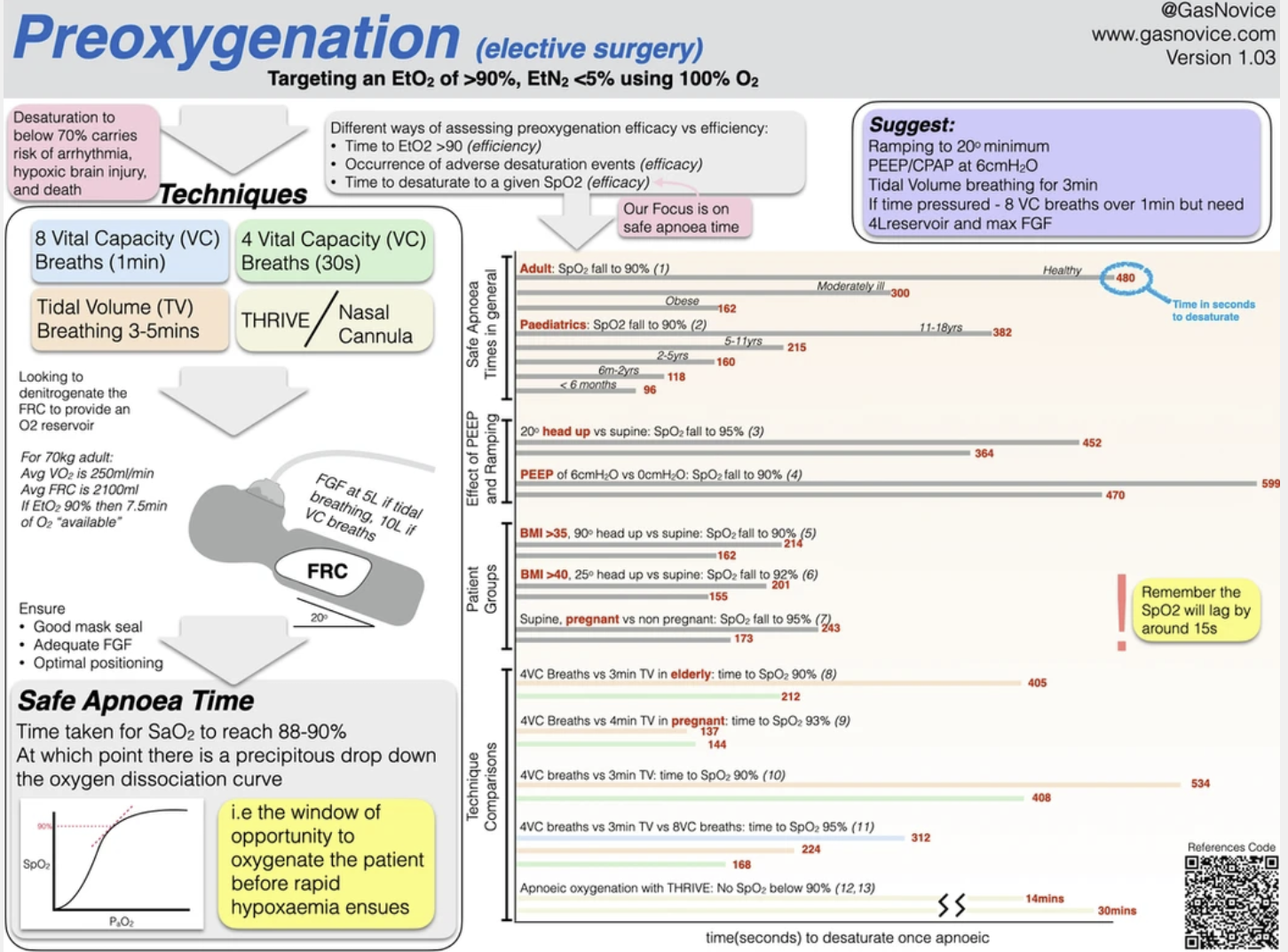
A great infographic
Tap the infographic below to head over to www.gasnovice.com to see all of their wonderful images and videos in full size and resolution.
References and Further Reading