Patient Controlled Analgesia

Take home messages
- PCA analgesia is safe and effective, but not without its side-effects
- You need to know all the safety features built into the set up
- Make sure your patient is actually able to use it
What is it?
Technically speaking, PCA or patient-controlled analgesia refers to any situation where a patient can decide (within reason) how much analgesic medication they receive and when.
Such as:
- A patient post-laparotomy with an intravenous morphine PCA pump
- A woman on labour ward pressing the button to trigger a bolus from her epidural pump
- A teenager in resus sipping on entonox while they have their shoulder relocated
These are all forms of patient-controlled analgesia, however when we say 'PCA' we usually mean the first - intravenous opioids.
So let's bash through some of the most common and high yield exam questions assuming that this is what we're talking about.
What pain relief options are available in the immediate post operative period?
- Simple regular analgesia - paracetamol
- NSAIDs where not contraindicated - we don’t use these enough
- Weak opioids - codeine
- Strong opioids - oral, IM, IV, PCA
- Adjuncts - gabapentin, amitriptyline
- Miscellaneous - lidocaine, ketamine, clonidine
- Regional analgesia
- Neuraxial analgesia
What are the side effects of opioids?
- Nausea
- Vomiting
- Hallucination or confusion
- Respiratory depression
- Pruritus
- Constipation
Make sure you also prescribe a laxative, chlorphenamine and naloxone PRN.
What are the advantages of patient controlled analgesia?
- Rapid strong analgesia on demand
- Gives the patient control and they don’t have to wait for the nurse to be free
- Reduced work load for nursing staff
- No painful IM or SC injections
Do not underestimate just how powerful a sense of control can be for improving a patient's pain. Simply knowing that they can press it whenever they need often has a placebo effect all by itself.
How would you initiate a PCA pump regime?
- Confirm patient identity and indication
- Rule out allergies and contraindications - renal failure and morphine etc
- Explain it to the patient, ideally with written information as well
- Check the patient is capable of understanding and using the button
- Ensure dedicated IV access
- Prescribe PRN oxygen, naloxone, chlorphenamine, laxatives
- Choose a PCA drug (morphine, fentanyl, ketamine, oxycodone)
- Select the dosing regime needed
- Sign the relevant documentation to ensure correctly set up, and watch patient administer first dose
- Monitor for adverse reactions
This is weirdly high yield in the exam, they really want to check that you understand the detailed set up protocol, because this is what makes it safe and effective.
Describe how a PCA pump works
- The idea is simple negative feedback - when the patient is in pain, they press for more analgesia, and when they’re comfortable, they don’t
- This naturally prevents over and under dosing and ensures a safe therapeutic level is maintained
- Different patients need different amounts, and a PCA pump allows the individual to titrate to their own requirements
- It is a computerised, battery powered and programmable pump that stores user data using a microprocessor
- When the pump is pressed, a predetermined dose of drug is administered through a dedicated intravenous line
- A time then locks the pump for a set duration, to prevent the patient from overdosing by administering too frequently
There are two options:
- Bolus only, with lockout in between
- Background infusion with boluses for breakthrough pain
The duration of the lockout should approximate the time to peak drug effect to prevent dose stacking.
Background infusions of intravenous opioids are usually reserved for the hallowed grounds of HDU and ICU.
What safety features are present in a PCA pump?
- The drug bag should be a dedicated PCA mixture at a set concentration designed only for PCA use
- The pre-programmed infusion regimes are double checked by the user prior to starting
- The pump will not give more than 85-90% of the volume of the bag, to prevent venous air embolism
- One way valves to prevent venous back flow
- Dedicated cannula
- Pumps have alarms for occlusion, air bubbles or empty bag
- The pump case should be lockable to prevent others tampering with the drug
What are the programmable parameters of a PCA pump?
- Bolus dose
- Lockout interval
- Dose limits
- Infusion rates
Usually these are pre-programmed into a given protocol that you select for whatever bag of drug you're plumbing into the pump.
What are the patient factors that increase risk with PCA?
- Elderly patients
- Obstructive sleep apnoea
- Concurrent sedatives/opioids
- Hypovolaemia
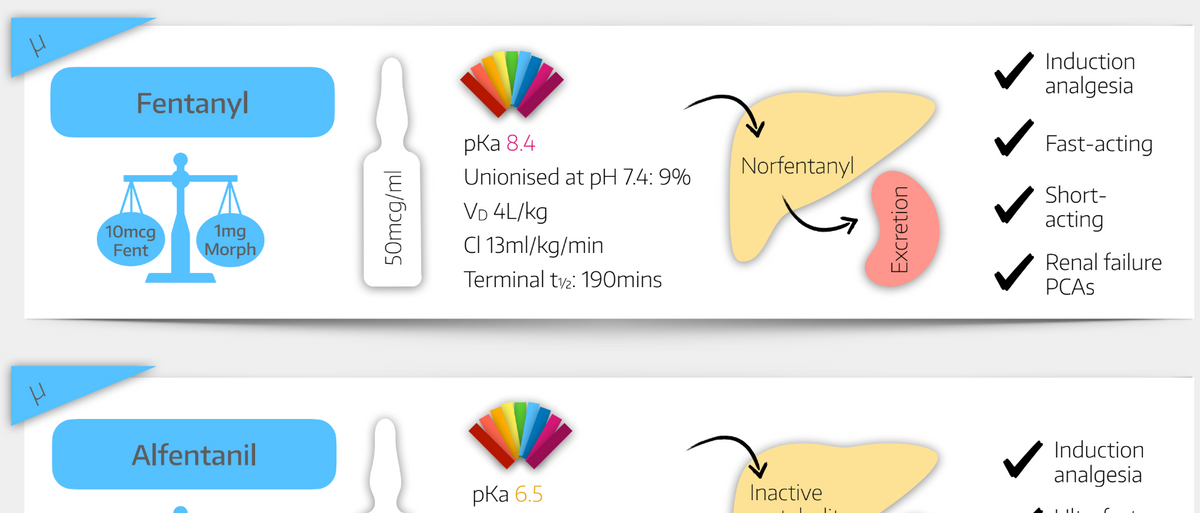
- Renal failure - use fentanyl rather than morphine
What instructions should be given to the ward nurse after setting up a PCA?
- There should be a specific PCA monitoring proforma to adhere to
- Sedation scoring and respiratory rate monitoring to monitor for opioid overdose
- Patient may need O2 therapy while on PCA
- Call the pain team or anaesthetist on call if any issues
Sedation precedes respiratory depression and is a better indicator of opioid toxicity than respiratory rate.
What doses would you use for an IV opioid PCA?
- Morphine 0.5 - 2mg with 5 - 10 minute lockout
- Fentanyl 10 - 50 mcg with 5 - 10 minute lockout
- Oxycodone 0.5 - 1 mg with 5 - 10 minute lockout
- Pethidine 5 - 20 mg with 5 - 15 minute lockout
You could also mention remifentanil which is increasingly available on labour ward as a 20 - 40 mcg bolus every 2 minutes. This is such short-acting analgesia that it's only really helpful for contraction pain so it isn't used anywhere else in the hospital.
Which patients should not be started on a PCA pump?
- Patients with dementia or delirium who lack capacity to use it properly
- Very young patients (unless supervised appropriately)
- Patients at risk of abuse where others may press the button for them
What other PCAs do you know of?
- Epidural
- Peripheral nerve catheter
- Subcutaneous
- Transdermal
These are specifically the 'push button to get a dose of drug' PCAs. You could also mention the examples we mentioned at the beginning where the patient determines how much pain relief they receive.
It's not the golden ticket
You can't just see a patient in pain and whack them straight onto a PCA without thinking about it properly, because they don't work for everyone and they carry significant side effects.
- Think about the other analgesia techniques you can employ first
- See if you can avoid opioids altogether, as we know this usually helps
- Make sure the patient understands how it works and is actually able to use the pump before you prescribe it
- Make sure nobody else is going to press the button for them
And as a final thought, if a patient's analgesic requirement appears to be steadily increasing, it's worth exploring why as simply increasing the PCA dose can mask new pathology, such as compartement syndrome, urinary retention or even an infarction.
Useful Tweets
@hdswoboda
— Dr. Naveen Eipe, MD (@NaveenEipe) June 15, 2023
We routinely add ketamine to opioids for delivery via patient-controlled analgesia #PCA
The indications for using ketamine #UltraLowDose in acute pain are similar? #SelfCitation
From https://t.co/dG2HQLi5XY pic.twitter.com/6skafD7nd0
References and Further Reading


Primary FRCA Toolkit
Members receive 60% discount off the FRCA Primary Toolkit. If you have previously purchased a toolkit at full price, please email anaestheasier@gmail.com for a retrospective discount.

Discount is applied as 6 months free membership - please don't hesitate to email Anaestheasier@gmail.com if you have any questions!
Other useful posts

Just a quick reminder that all information posted on Anaestheasier.com is for educational purposes only, and it does not constitute medical or clinical advice.