Breathing Circuits
The Mapleson Circuits
💡
This is a classification of semi-open, rebreathing systems with no CO2 reabsorption when used correctly.
Each circuit has a different arrangement of fresh gas supply, reservoir bag, APL valve and tubing, with consequently different characteristics. They are classified from A to F.
You'll probably only really use C and D.
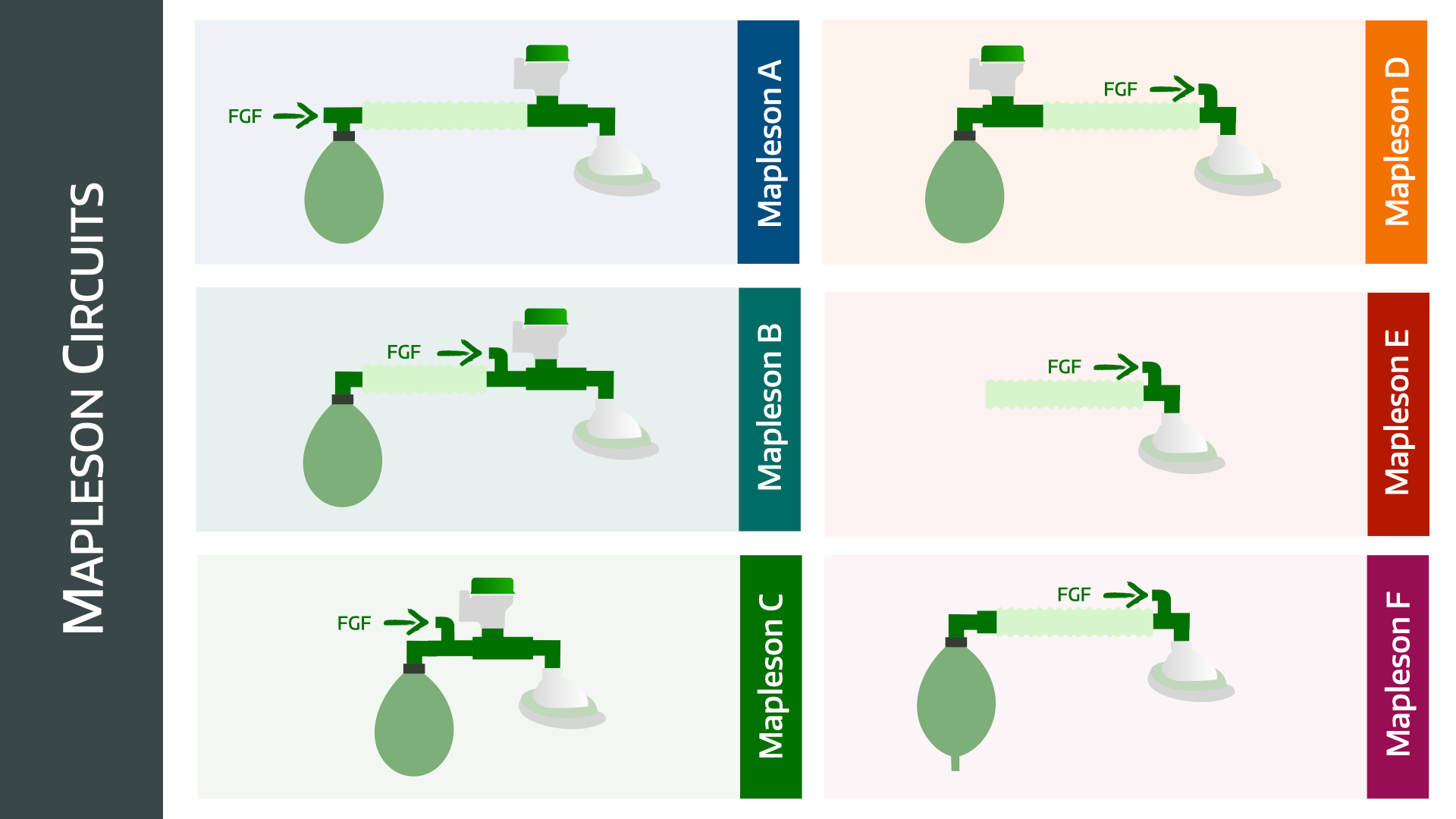
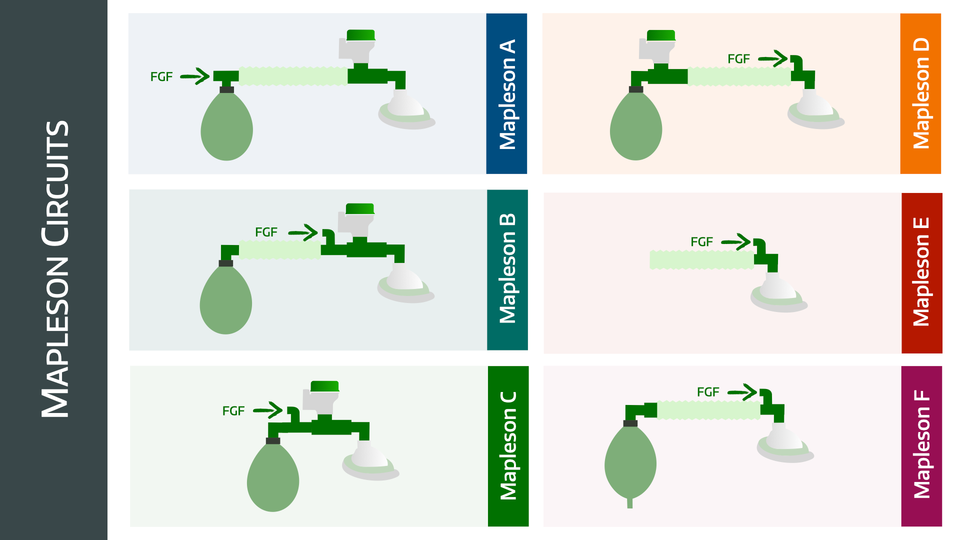
Mapleson A
- The bag is right next to the fresh gas flow, and the APL valve is next to the patient at the other end of the corrugated tubing
- It is very efficient for spontaneous breathing, because the exhaled gas is pushed quickly out of the APL valve by the patient
- It is terribly inefficient for controlled ventilation, because there isn't enough expiratory pressure to push the exhaled gas out, unless you have high fresh gas flows
- There is a co-axial version called the Lack circuit
Mapleson B
- Similar to the Mapleson A, however the fresh gas flow is now at the patient end
- It's rubbish for everything, don't use it
Mapleson C
- This is a Mapleson B without the corrugated tubing
- In order it goes bag-fresh gas flow-APL-patient
- It's still very inefficient, however its compactness makes it useful for resuscitation
Mapleson D
- Also has a co-axial version known as the Bain circuit
- This is essentially a Mapleson A with the APL and fresh gas flow switched around
- Bag - APL - corrugated tubing - fresh gas - patient
- This is much more efficient for controlled breathing, as the fresh gas flow right next to the patient means the exhaled gas is quickly pushed down the tubing to the bag and apl valve
- It's very inefficient for spontaneous breathing because the shorter expiratory time means the patient ends up drawing exhaled gas back in before it can be pushed out the way
Mapleson E
- This is a weird contraption with no bag or apl valve
- It's the T-piece they hand you to stick on the IGEL before you head to recovery
- You can only use it for spontaneous breathing, and it's not very efficient
Mapleson F
- Also known as the Jackson Rees modification
- It is the Mapleson E circuit with a bag attached at the end of the corrugated tubing, but the bag has a hole in it
- The hole can be used as a manual APL valve/PEEP valve
- Used a lot in paediatrics
- There is another version of the Mapleson F that has an APL valve instead
High Yield Questions for the Primary FRCA
What are the different types of anaesthetic breathing systems?
Breathing systems can be classified as open, closed, semi-open and semi-closed
Open
- The patient's airway is completely open to the atmosphere
- An example would be breathing room air through a cloth soaked in vapour to provide anaesthesia (open drop ether mask)
- There is no reservoir bag, no rebreathing of exhaled gas, no tubing or valves
Semi-Open
- Semi-open systems have a reservoir bag
- No functional re-breathing of exhaled gases
- High fresh gas flows
- Mapleson breathing systems
Semi-Closed
- Reservoir bag
- Partial re-breathing of exhaled gases
- Unidirectional valves
- CO2 absorption
- Includes circle system with APL valve open
Closed
- The patient's airway is completely isolated from the atmosphere
- Complete functional rebreathing of exhaled gas
- An example would be a circle circuit with the APL valve closed and a flow low enough so as not to disturb the exhaust valve
What are the properties of an ideal breathing system?
- Easy to use
- Inexpensive components
- Reliably delivers the correct mixture of inspired gases
- Allows for both controlled, manual and spontaneous ventilation
- Suitable for all patient ages
- Efficient, allowing low fresh gas flow
- Safe, protecting patient from barotrauma
- Strong, compact and lightweight
- Facilitates scavenging of anaesthetic gases
- Minimal maintenance or running cost
Tell me about the Bain Circuit
This is the coaxial Mapleson D
- The setup of a Bain circuit means it behaves differently for spontaneous and mandatory ventilation
- Spontaneous ventilation is very inefficient as it allows for significant rebreathing unless there is a high fresh gas flow of 150-250ml/kg/min or approximately 3x minute ventilation
- Controlled ventilation, however, is efficient as the waste alveolar gas is vented through the APL valve, but the dead space gas collects in the reservoir bag and is used again
- This allows fresh gas flow to be as low as 70ml/kg/minute
What is the main risk with a co-axial mapleson B or Bain circuit?
- Disconnection of the inner tube supplying fresh gas flow. This converts the entire circuit into dead space and causes significant rebreathing of CO2
Can you explain why the Mapleson A circuit is better for spontaneous breathing than controlled ventilation?
- During spontaneous expiration, the corrugated tubing is filled with dead space gas (with minimal CO2) from the patient end, and fresh gas flow from the machine end fills the reservoir bag
- As long as fresh gas flow matches alveolar ventilation, then by the time the CO2-rich alveolar gas is exhaled, then the system will be full and the pressure increases, and thus the excess gas will be vented out of the APL valve
- However during controlled ventilation, the pressure during expiration remains low enough that the alveolar gas is not vented out through the APL valve, and is therefore re-breathed unless the fresh gas flow is at least three times alveolar minute ventilation
What are the four functions of the bag?
- Collects fresh gas during expiration, to serve as a reservoir for the next breath
- Adult standard size is 2 litres
- Paediatric bags are usually 0.5 litres
- The Mapleson F system employs a double-ended bag that also serves as the expiratory port and PEEP valve
- Up to 6 litre bags exist
- Visual monitor of spontaneous ventilation
- Manual support or control of ventilation
- Distends under pressure, preventing barotrauma to the patient
What does the APL valve do?
- The APL valve is an adjustable, spring-loaded, one way valve
- Acts as a safety pressure limiter
- When pressure in system exceeds the set pressure, it allows gas to escape
- In the closed position, most APL valves have a pressure limit of 60-70kPa to prevent barotrauma to the patient
- In the open position it requires a pressure of less than 0.1kPa to open
- Generates PEEP
- May or may not have scavenging attached
Describe the Circle breathing system
The circle breathing system is a semi-closed, rebreathing system with CO2 absorption that is commonly incorporated into the anaesthetic machine.
The key components of the circle breathing system are as follows:
- Inspiratory and Expiratory valves
- Wide-bore corrugated tubing
- CO2 absorbing soda lime cannister
- Reservoir bag
- Adjustable Pressure Limiting (APL) valve
Advantages
- Very efficient for both spontaneous and mandatory ventilation
- Cost effective and allows very low gas flows, preserving vapour
- Easy to retain warmed humidified gases with HME filter
- Facilitates monitoring of anaesthetic gases
Disadvantages
- Bulky
- Higher resistance to respiratory effort than some circuits
- Multiple components that can fail
- Potential risk of hypoxic mixtures due to rebreathing
- Some agents cause carbon monoxide production as they pass through a warm, dry CO2 absorber, particularly baralyme
- Some other substances can accumulate in the system
- Compound A (from sevoflurane)
- alcohol if patient intoxicated
- methane and hydrogen from bacteria in the patient
For a full breakdown of why the Mapleson systems behave the way they do, check out this review
Medical Pharmcology: Physics and Chemistry in Anesthesiology, Breathing Circuits
Breathing circuits including Mapleson systems are discussed.
