Breathing Systems
In the bad old days, when a 'balanced anaesthetic' consisted of one person holding each limb, and a slug of whisky with a leather rag to bite on if you were lucky, the most popular breathing system in use was the patient's own respiratory tract, connected through a native airway to atmospheric air.
Since adrenaline is a fiercely powerful bronchodilator and screaming usually generates rather decent tidal volumes, presumably very few patients died of hypoxia (before they died of something else).
Thankfully, times have changed.
With the advent of anaesthetic agents that actually work, providing the ability to spare our patient the horror of vivisection, we have also added in a few other effects that we need to contend with:
- Depression of respiratory drive
- Relaxation of muscle tone and airway obstruction
- Ventilation/perfusion mismatch
- Myocardial depression and vasodilatation
So we need airway devices and breathing systems to help us manage these issues.
What is a breathing system?
The problems that a breathing system solves are:
- How do I know how much oxygen I'm giving my patient?
- How much anaesthetic agent am I giving my patient?
- How much nitrous oxide is being delivered?
- How do I make sure they're getting rid of enough CO2?
So any tubing, reservoir bag, valves and CO2 scavenging systems are all part of the breathing system.
What are the different types?
Regardless of what breathing system you're using, it's going to contain the same fundamental elements:
- A fresh gas flow supply
- A connection to the patient
- An inspiratory limb
- An expiratory limb
- An expiratory valve or port
They may then also have a reservoir bag, some sort of CO2 absorption mechanism, and corrugated tubing to connect everything together.
What are the properties of an ideal breathing system?
- Easy to use
- Inexpensive components
- Reliably delivers the correct mixture of inspired gases
- Allows for both controlled, manual and spontaneous ventilation
- Suitable for all patient ages
- Efficient, allowing low fresh gas flow
- Safe, protecting patient from barotrauma
- Strong, compact and lightweight
- Facilitates scavenging of anaesthetic gases
- Minimal maintenance or running cost
Open vs Closed
This gets examined. It also gets people confused because it's not a very intuitive way to divide breathing systems into groups.
The way I like to understand this classification is with three questions.
- Is the patient supposed to rebreathe their expired gases?
- If no - does the system have a reservoir bag?
- If yes - how much of their expired gases are they supposed to be inhaling?
The combination of answers will lead you to one of the following options:
Open
Open breathing systems have:
- No reservoir bag
- No rebreathing
- No tubing
- No valves
Examples include Schimmelbusch open drop masks.
You know those ones you use every Thursday on your gynae list with Dr Roberts...
Semi-open
Semi-open systems have:
- Reservoir bag
- No rebreathing
- Needs high fresh gas flow to flush out CO2
Examples include the Mapleson systems.
Semi-closed
Semi-closed systems have:
- Reservoir bag
- Partial rebreathing of exhaled gases
- Unidirectional valves
- CO2 absorbers
- Lower fresh gas flows
Examples include the circle system with the adjustable pressure limiting (APL) valve open at least a little bit.
Closed
Closed breathing systems have:
- Reservoir bag
- Total rebreathing of exhaled gases
- CO2 absorbers
- Lowest fresh gas flows
Examples include the circle system with the APL valve closed.
If that doesn't make sense, hopefully this video does.
The Mapleson Circuits
This is the highest yield bit for the exams, it comes up a lot.
William Mapleson spent a large chunk of 1954 sticking tubes, valves and bags together in different arrangements to see how they behaved.
- An FGF inlet delivers the desired mixture of oxygen, air and anaesthetic agent into the breathing system
- The pressure starts to build (assuming it's connected to a patient) in the system
- Once the pressure exceeds the set value, the APL valve opens
- This allows gases to exit the breathing system
- An open APL valve allows all expired gases to exit the system, as it only takes around 1 cmH2O of pressure to open
- Closing the APL valve allows continuous positive airway pressure (CPAP) to be delivered to a spontaneously breathing patient
- If you want to squeeze the bag to give the patient a mandatory breath, you need to close the APL valve to at least the pressure needed to inflate their chest
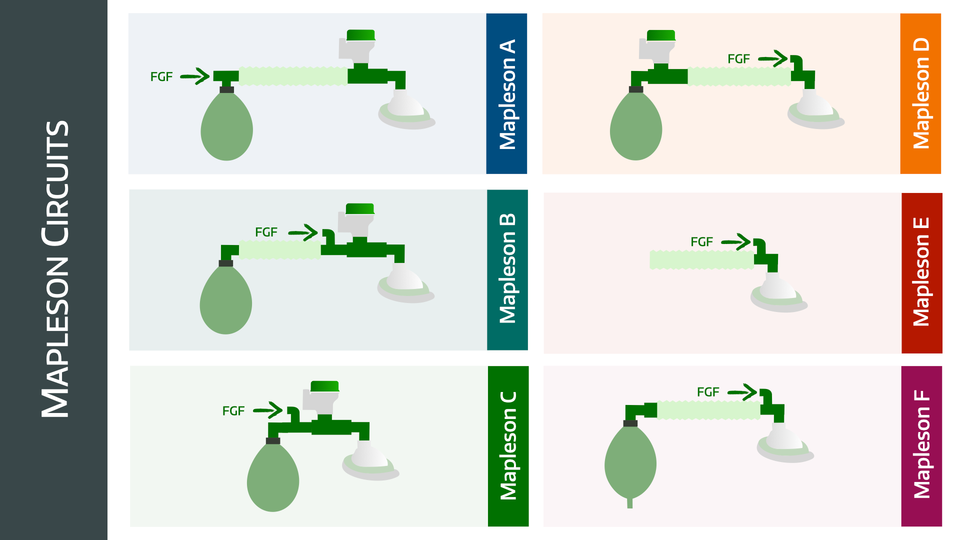
Each circuit has a different arrangement of fresh gas supply, reservoir bag, APL valve and tubing, with consequently different characteristics. They are classified from A to F.
Here they are
You probably won't find yourself using A or B clinically, but the others do feature in the real world.
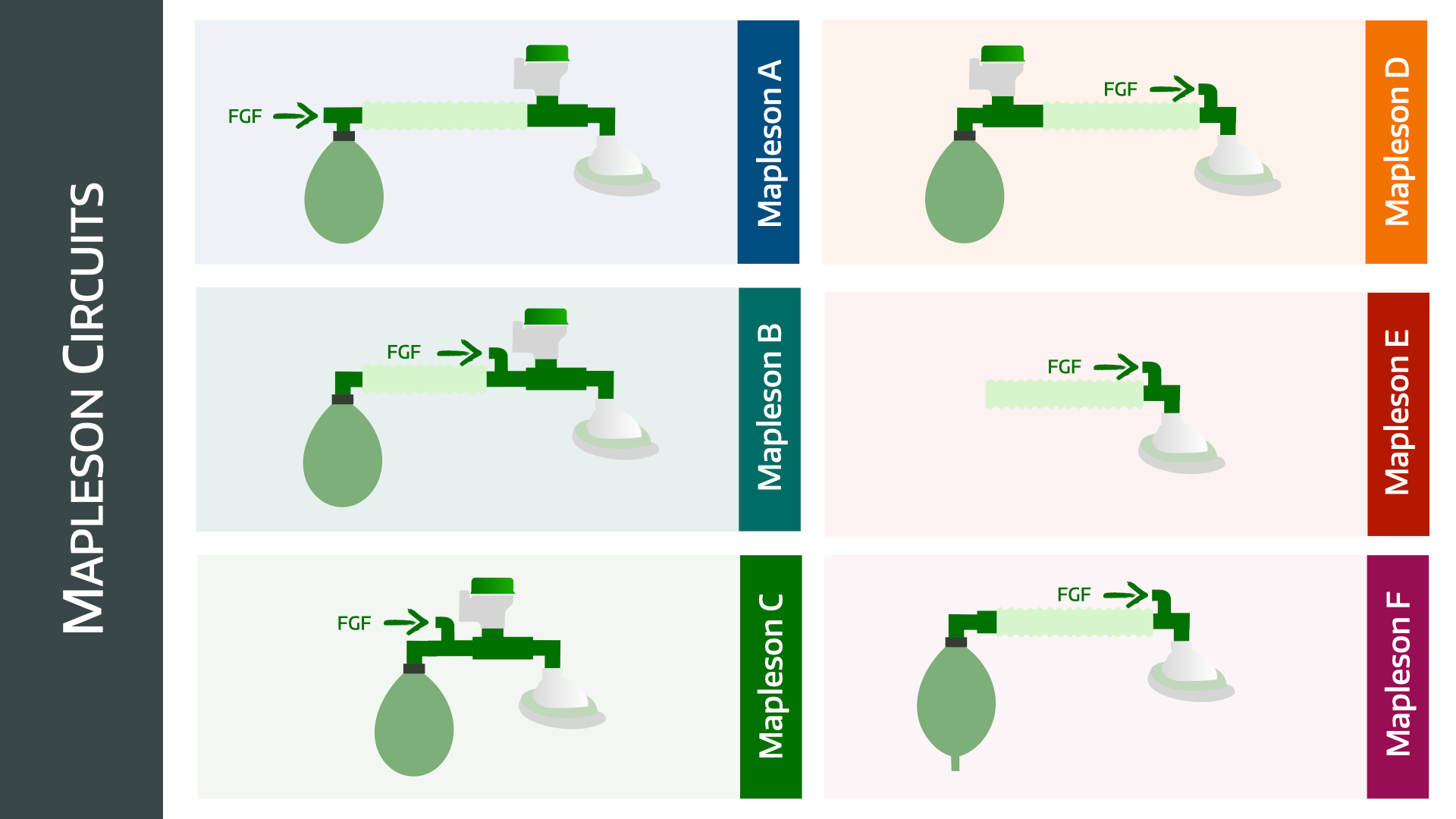
Mapleson A
- Also called the Magill system
- The bag is right next to the fresh gas flow, and the APL valve is next to the patient at the other end of the corrugated tubing
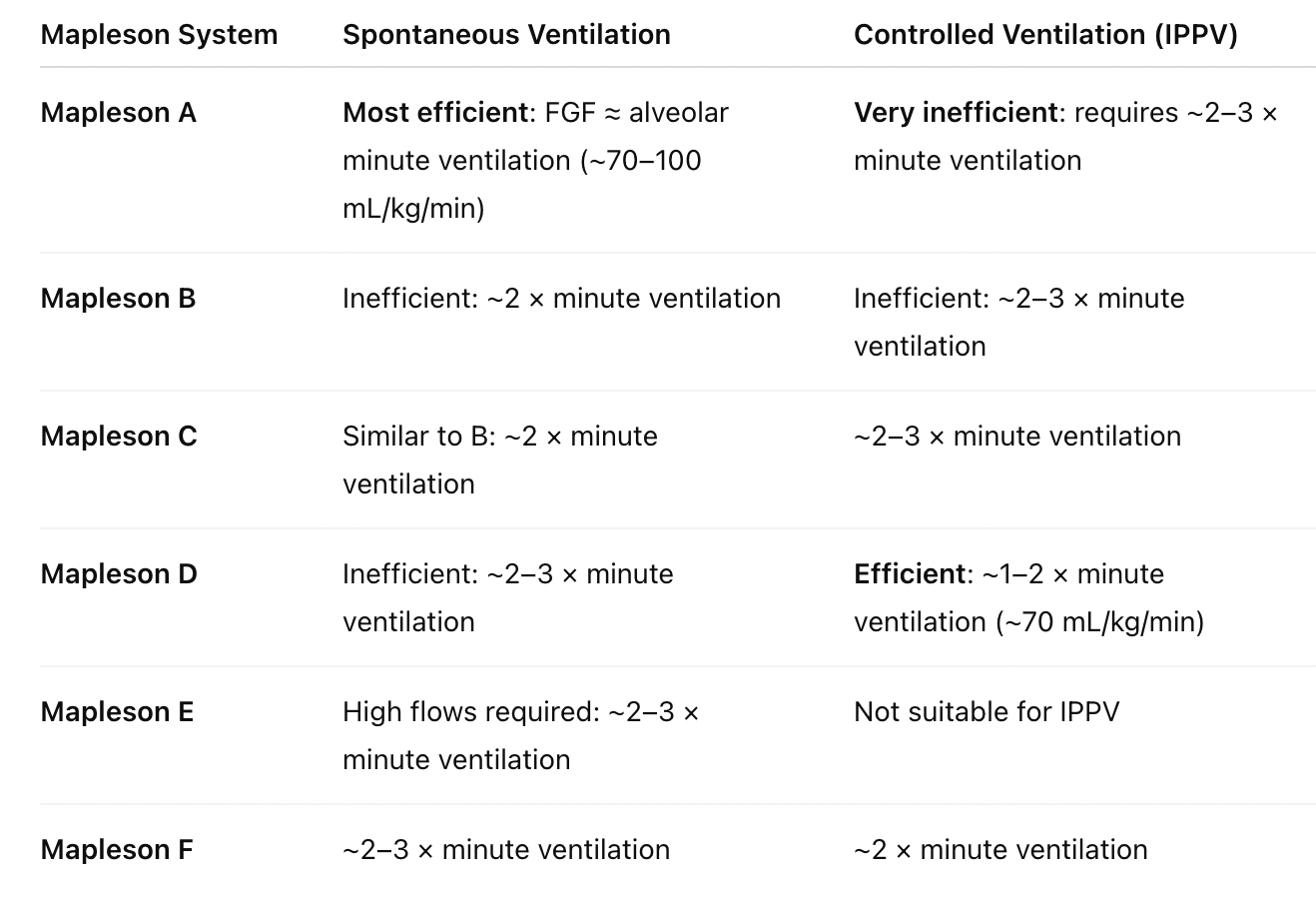
- It is very efficient for spontaneous breathing, because the exhaled gas is pushed quickly out of the APL valve by the patient
- It is terribly inefficient for controlled ventilation, because there isn't enough expiratory pressure to push the exhaled gas out, unless you have high fresh gas flows
- There is a co-axial version called the Lack circuit
Mapleson B
- Similar to the Mapleson A, however the fresh gas flow is now at the patient end
- It's rubbish for everything, don't use it
Mapleson C
- This is a Mapleson B without the corrugated tubing
- In order it goes bag-fresh gas flow-APL-patient
- It's still very inefficient, however its compactness makes it useful for resuscitation
Mapleson D
- Also has a co-axial version known as the Bain circuit
- This is essentially a Mapleson A with the APL and fresh gas flow switched around
- Bag - APL - corrugated tubing - fresh gas - patient
- This is much more efficient for controlled breathing, as the fresh gas flow right next to the patient means the exhaled gas is quickly pushed down the tubing to the bag and APL valve
- It's very inefficient for spontaneous breathing because the shorter expiratory time means the patient ends up drawing exhaled gas back in before it can be pushed out the way
Mapleson E
- This is a weird contraption with no bag or APL valve
- It started out as the Ayre's T-Piece which you can read about here
- It's the T-piece they hand you to stick on the IGEL before you head to recovery
- You can technically generate positive pressure by occluding the exhaust tube but it's not exactly scientific
- The main benefit is the exceptionally low resistance due to the lack of components, making it useful for spontaneously breathing children
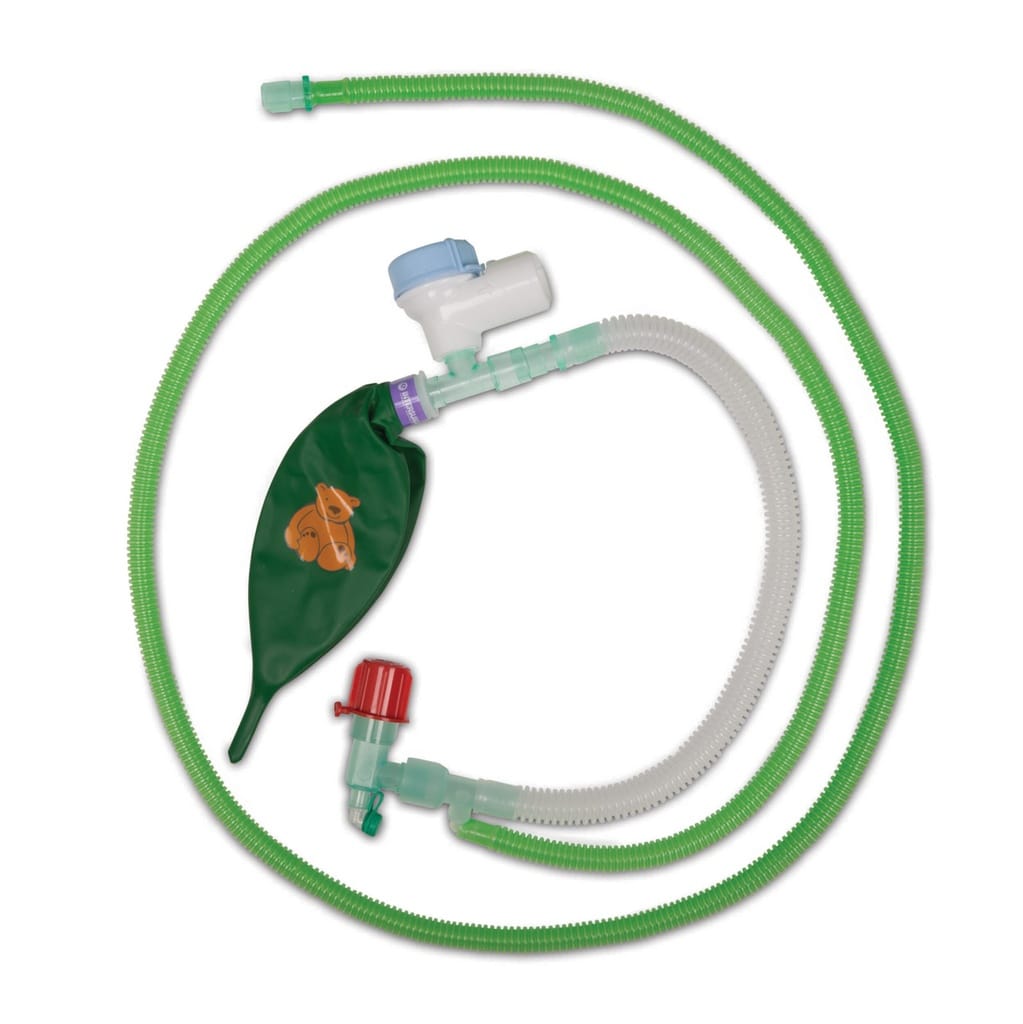
Mapleson F
- Also known as the Jackson Rees modification
- It is the Mapleson E circuit with a bag attached at the end of the corrugated tubing, but the bag has a hole in it
- The hole can be used as a manual APL valve/PEEP valve
- Used a lot in paediatrics
- There is another version of the Mapleson F that has an APL valve instead
What fresh gas flow do I need?
Why is a Mapleson A so much better for spontaneous than controlled ventilation?
YES.
Most people just memorise this, and don't actually understand why it happens.
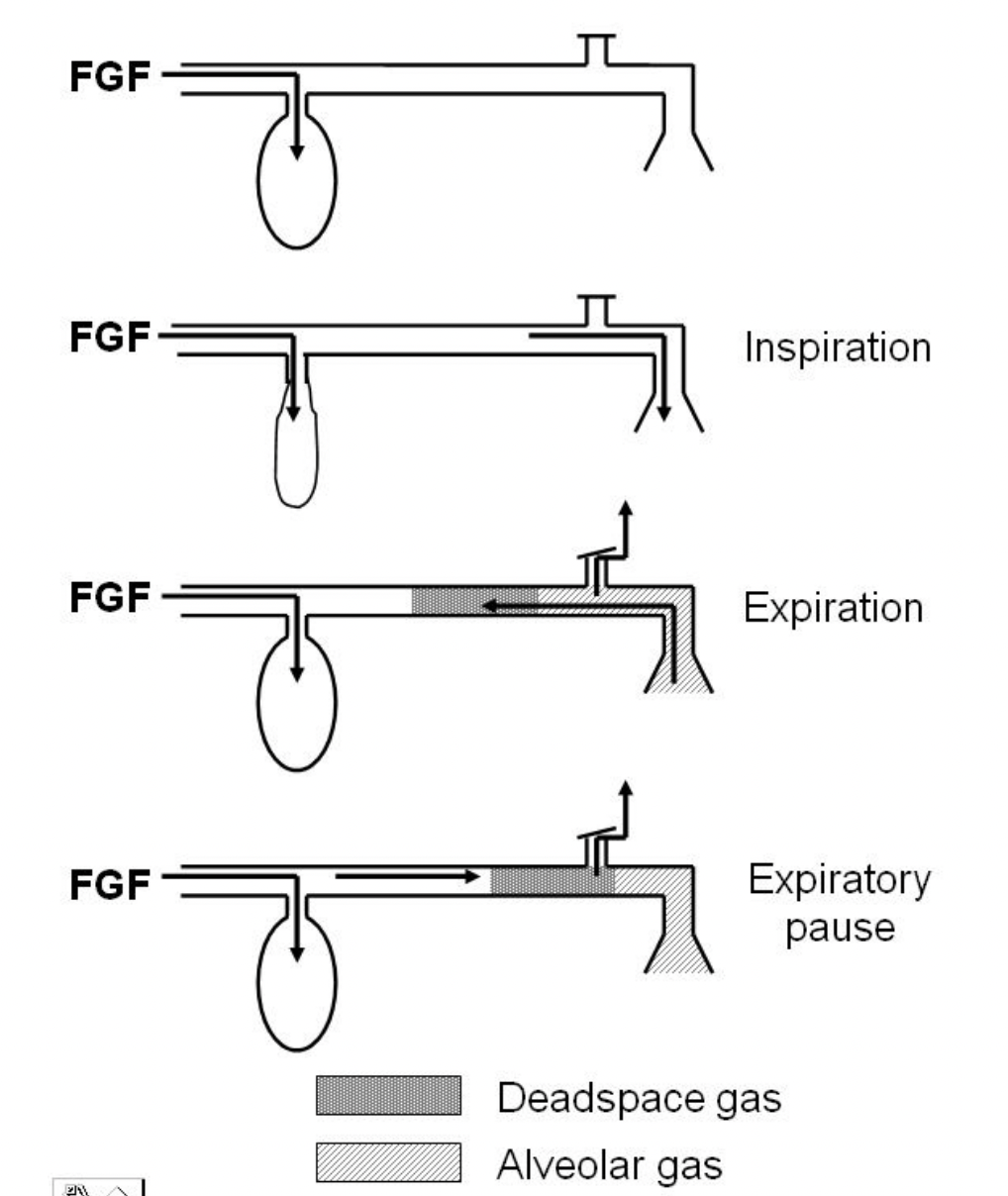
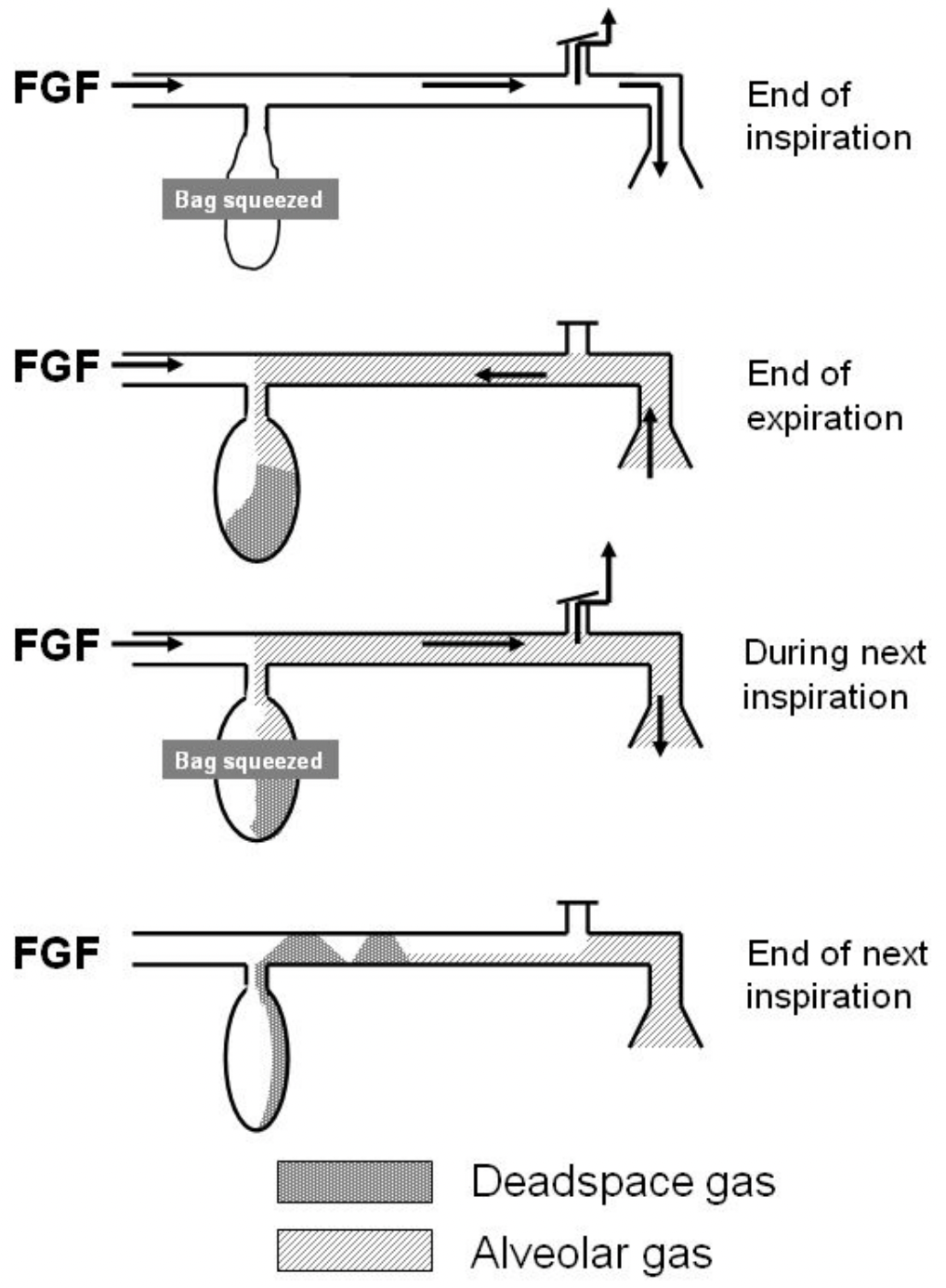
Spontaneous ventilation
When breathing spontaneously, with the APL valve open:
- The patient inhales
- The system is continually topped up with fresh gas from the other end
- The patient exhales their dead space gas into the breathing system
- This is followed by the alveolar gas (containing CO2)
- By this point the reservoir bag has already filled up with fresh gas and so the pressure in the breathing system rises enough to open the APL valve
- Conveniently, the APL valve is at the patient end
- This means the exhaled alveolar gas is allowed to escape
- The continued influx of fresh gas from the other end helps push it out
- The patient then breathes in again
Technically the patient is allowed to breathe the dead space gas back in again, so you technically only need to match their alveolar minute ventilation, but in reality people target the total minute ventilation just for a bit of a buffer.
Controlled ventilation
Here everything changes because you need to have the APL valve at least slightly closed in order to generate enough pressure to inflate the patient's lungs
- You squeeze the bag full of fresh gas, generating positive pressure
- Some of the fresh gas flow inevitably gets shoved out of the APL valve
- The patient exhales
- Because you've emptied the fresh gas flow from the bag, the patient's exhaled alveolar gas is free to track back along the system and fill the bag
- The next breath you give will then have CO2 in it
The only way to prevent this is with really high fresh gas flows to flush the system through every breath.
Okay, so is it the same thing for why Mapleson D systems are worse for spontaneous breathing?
Sort of.
Why Mapleson D is rubbish for spontaneous breathing
All three of the Mapleson D, E and F systems are essentially a glorified T piece with the fresh gas flowing in at the patient end of the system, compared to the machine end as in the Mapleson A.
If you allow the patient to breathe spontaneously:
- The exhaled gas and new fresh gas will mix in the tubing
- This mixture travels towards the reservoir bag and APL valve
- When the bag fills and APL valve opens, you lose a mixture of fresh and exhaled gas into the atmosphere
- During the next breath, the patient inhales a mixture of new fresh gas and left over exhaled gas that's still in the tubing
Unless you have at least 8 to 10 litres per minute of fresh gas flow.
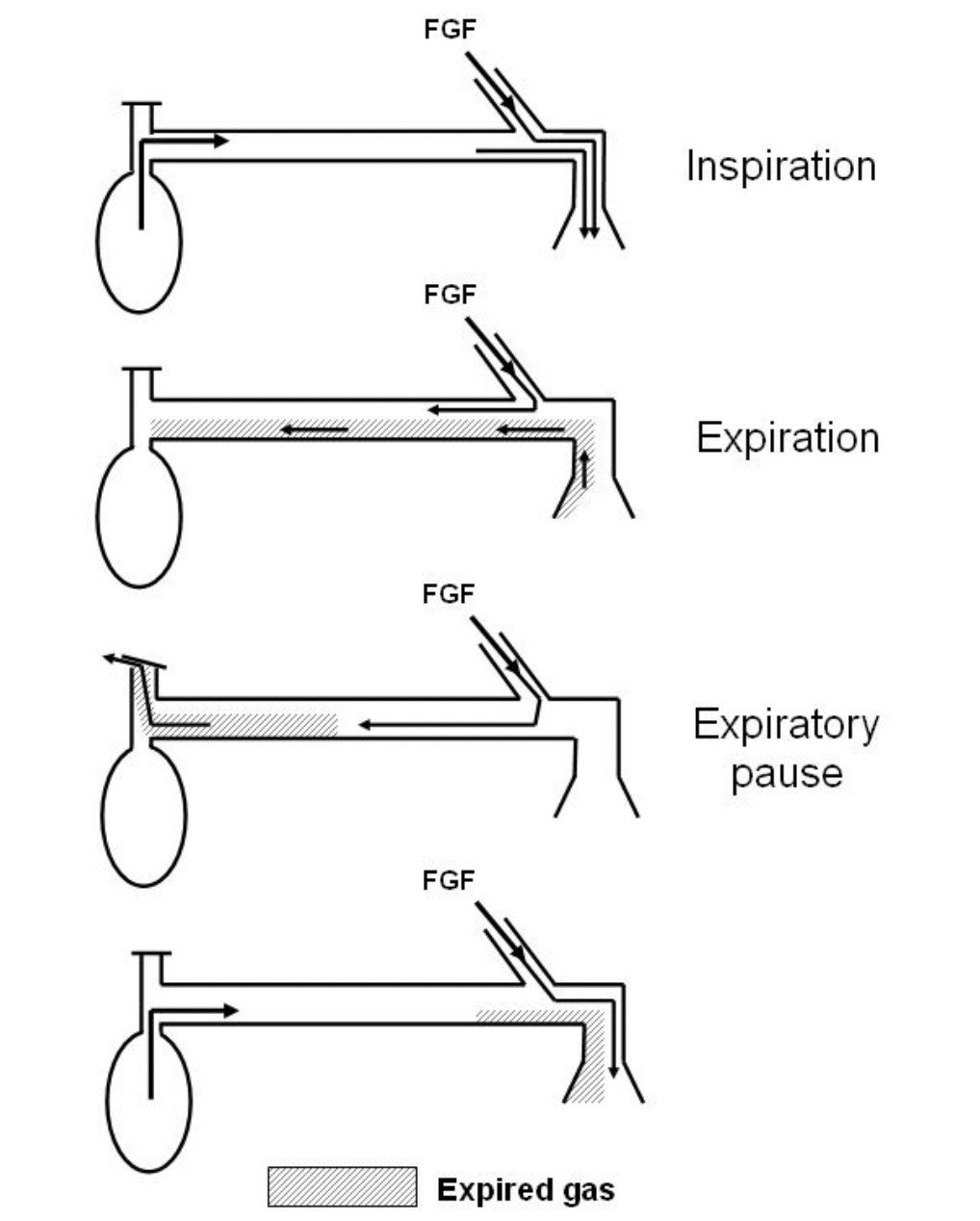
During controlled ventilation however:
- The APL valve is at least partly closed
- You squeeze the bag to generate a tidal breath
- Some gas escapes through the APL valve
- The bag collapses
- You can't give another breath until the bag fills up
- This means there is a much longer expiratory pause than with spontaneous breathing
- This allows the exhaled gas to be pushed along into the bag by the new fresh gas flow
Then when you next squeeze the bag (full of exhaled CO2), the tubing is full of fresh gas for the patient, and when the APL valve opens right next to the bag, your exhaled CO2 is allowed to escape.
So in summary:
- The efficiency of the Mapleson A depends on the ability of the bag to fill with enough fresh gas, to generate sufficient pressure to open the APL valve at the patient end
- The efficiency of the Mapleson D depends on the ability of the fresh gas flow to push the exhaled gas along to the bag during the expiratory pause
Easy.
What the hell is this?


The Humphrey Breathing System
I'll be amazed if you ever use this. I'll be less surprised if you get examined on it.
- A mechanical valve system that allows the operator to convert the breathing system between a Mapleson A, D or E just by moving a lever
- Mapleson A is most efficient for spontaneous breathing
- Mapleson D is most efficient for IPPV
- Mapleson E facilitates low-pressure ventilation of the spontaneously breathing patient
- The circuit consists of a metal block with a fresh gas inlet, two reservoir bag connectors, an APL valve, tubing connectors and rotary valves connected to the selector lever
- The selector lever moves the rotary valves which in turn alter the dynamics of the circuit to be either a Mapleson A, D or E system
- It is either a semi-open or a semi-closed system, depending on whether it is set up as a circle system with soda lime
You absolutely do not need to know any more about it than that.
So why a circle?
We have two main problems with conventional breathing systems:
- Every time the patient exhales, all of the anaesthetic gas and unused oxygen is being lost into the atmosphere
- The fresh gas flow needs to be high enough to flush out the patient's exhaled CO2, which makes the first problem even worse
The circle system aims to solve both of these issues.
How?
By recycling.
Every molecule of exhaled oxygen and sevoflurane is perfectly safe to use again, so they're sent round the circle to be inhaled once more.
- This massively reduces the amount of sevoflurane that is used and therefore flushed out into the atmosphere
- It also reduces how much oxygen is wasted, because if you're using the circle correctly you only need to replace what the patient consumes
By adding in a canister of soda lime or equivalent, you can then soak up those pesky exhaled CO2 molecules.
How low can you go?
When you're preoxygenating your patient with a circle system, you're going to have your FiO2 set to 100% and your flows high at 10 - 15 litres per minute.
If you left them like this for the whole case then you are still using a circle breathing system, you're just using it really badly.
Kind of like driving a racecar in second gear for the whole lap.
The whole point of a circle system is low flow anaesthesia, dropping your fresh gas flow as low as safely possible, in order to minimise how much oxygen, sevo and nitrous are lost into the atmosphere.
How does that work?
- If your patient is spontaneously ventilating and the ventilator is switched off, then the APL valve will determine at what pressure excess gas is allowed to escape the circle system
- If the ventilator is working, then it will vent anything that exceeds the inspiratory pressure during the inspiratory phase and the PEEP during the expiratory phase
- If your fresh gas flow is higher than the rate of oxygen consumption, the volume of gas in the system will gradually increase
- At some point the pressure will build above the setting on the APL valve, or the ventilator, and the excess will be released
A perfect low-flow circle system would see your fresh gas flow replacing only the consumed oxygen, with no net addition of gas to the circle.
You can find a cool calculator here to see just how terrible we are for the environment:
Then you can make yourself feel better by going to Flight Radar and seeing just how many planes there are in the sky right now, and that your slightly sub-optimal anaesthetic probably isn't such a big deal.
What if I'm running TIVA?
Your breathing system is still important for management of oxygen and carbon dioxide levels, especially in cases such as:
- Laparoscopy where the patient will absorb CO2 from the abdomen
- Neurosurgery where tight CO2 control is needed for intracranial pressure
- ENT where CO2 control is needed to prevent excessive bleeding in the operative field
Volatile anaesthetic agents are so fantastically terrible for the atmosphere that the ultimate priority is minimising their release into the atmosphere when in use, so the flow just needs to be as low as physically possible.
However with TIVA, you can actually think about the environmental impact of other parts of your equipment, specifically your soda lime.
- The lower the flow, the harder your soda lime has to work, as you're not flushing CO2 out into the atmosphere
- This consumes the soda lime much more quickly
- The production and disposal of soda lime is, you guessed it, terrible for the environment
- A higher fresh gas flow reduces how quickly the soda lime is exhausted, so ends up being better for the environment over all.
By matching at least the patient's minute ventilation, you essentially flush out all of the CO2 and theoretically therefore don't need to use up any of the soda lime.
Any higher than this, however, and you needlessly use excess oxygen, for which the ecological cost of production is substantial.
*Technically speaking, it depends on a multitude of factors including
- electricity source
- oxygen production
- absorbent manufacture and disposal
- transport
- institutional supply chain
But that doesn't help you choose a fresh gas flow this afternoon.
If you want an insanely detailed rabbit hole on this specific topic, go to this article.
High Yield Questions for the FRCA exams
What are the different types of anaesthetic breathing systems?
Breathing systems can be classified as open, closed, semi-open and semi-closed
Open
- The patient's airway is completely open to the atmosphere
- An example would be breathing room air through a cloth soaked in vapour to provide anaesthesia (open drop ether mask)
- There is no reservoir bag, no rebreathing of exhaled gas, no tubing or valves
Semi-Open
- Semi-open systems have a reservoir bag
- No functional re-breathing of exhaled gases
- High fresh gas flows
- Mapleson breathing systems
Semi-Closed
- Reservoir bag
- Partial re-breathing of exhaled gases
- Unidirectional valves
- CO2 absorption
- Includes circle system with APL valve open
Closed
- The patient's airway is completely isolated from the atmosphere
- Complete functional rebreathing of exhaled gas
- An example would be a circle circuit with the APL valve closed and a flow low enough so as not to disturb the exhaust valve
Tell me about the Bain Circuit
This is the coaxial Mapleson D
- The setup of a Bain circuit means it behaves differently for spontaneous and mandatory ventilation
- Spontaneous ventilation is very inefficient as it allows for significant rebreathing unless there is a high fresh gas flow of 150-250ml/kg/min or approximately 3x minute ventilation
- Controlled ventilation, however, is efficient as the waste alveolar gas is vented through the APL valve, but the dead space gas collects in the reservoir bag and is used again
- This allows fresh gas flow to be as low as 70ml/kg/minute
What is the main risk with a co-axial mapleson B or Bain circuit?
- Disconnection of the inner tube supplying fresh gas flow
- This converts the entire circuit into dead space and causes significant rebreathing of CO2
Describe the Pethick test
This is the test to see whether the inner tube has become disconnected.
- Completely block the patient end of the breathing circuit
- Fully close the APL valve
- Use the oxygen flush valve to fill the reservoir bag
- Release the occlusion at the patient end while continuously pressing the oxygen flush
Say what you see:
- If the reservoir bag collapses, the inner tube is intact and the system is working
- If the reservoir bag doesn't deflate, there is a disconnection
This phenomenon occurs due to the Venturi effect. Oxygen flushing out of the inner tube 'sucks' gas from the expiratory limb with it, deflating the bag.
If the inner tube is disconnected, then the flush leaks into the outer tubing and either inflates the bag or prevents it from collapsing.
What are the four functions of the bag?
- Collects fresh gas during expiration, to serve as a reservoir for the next breath
- Adult standard size is 2 litres
- Paediatric bags are usually 0.5 litres
- The Mapleson F system employs a double-ended bag that also serves as the expiratory port and PEEP valve
- Up to 6 litre bags exist
- Visual monitor of spontaneous ventilation
- Manual support or control of ventilation
- Distends under pressure, preventing barotrauma to the patient
What does the APL valve do?
- The APL valve is an adjustable, spring-loaded, one way valve
- Acts as a safety pressure limiter
- When pressure in system exceeds the set pressure, it allows gas to escape
- In the closed position, most APL valves have a pressure limit of 60-70 cmH2O to prevent barotrauma to the patient
- In the open position it requires a pressure of less than 0.1 cmH2O to open
- Generates PEEP
- May or may not have scavenging attached
Describe the Circle breathing system
The circle breathing system is a semi-closed, rebreathing system with CO2 absorption that is commonly incorporated into the anaesthetic machine.
The key components of the circle breathing system are as follows:
- Inspiratory and Expiratory valves
- Wide-bore corrugated tubing
- CO2 absorbing soda lime cannister
- Reservoir bag
- Adjustable Pressure Limiting (APL) valve
Advantages
- Very efficient for both spontaneous and mandatory ventilation
- Cost effective and allows very low gas flows, preserving vapour
- Easy to retain warmed humidified gases with HME filter
- Facilitates monitoring of anaesthetic gases
Disadvantages
- Bulky
- Higher resistance to respiratory effort than some circuits
- Multiple components that can fail
- Potential risk of hypoxic mixtures due to rebreathing
- Some agents cause carbon monoxide production as they pass through a warm, dry CO2 absorber, particularly baralyme
Some other substances can accumulate in the system
- Compound A (from sevoflurane)
- Alcohol if patient intoxicated
- Methane and hydrogen from bacteria in the patient
For a full breakdown of why the Mapleson systems behave the way they do, check out this review

References and Further Reading


Other related posts
The Toolkits
Everything you need to smash the exams, all in one place.
Members Area

Just a quick reminder that all information posted on Anaestheasier.com is for educational purposes only aimed at trained professionals, and it does not constitute medical or clinical advice.
Anaestheasier® is a registered trademark.