Facial Trauma

Take home messages
- Don't be distracted from the other trauma
- Plan your extubation carefully
- Remember the physiological impacts of trauma, as well as anatomic
What are the common causes of facial trauma?
As you may expect, facial trauma is most commonly seen in young males.
- Fighting*
- Sport
- Road traffic incidents
- Falls
- Industrial accidents
*Examiners prefer interpersonal trauma.
What are your concerns for a patient with facial trauma?
It's easy to imagine, or look at, a patient with major facial trauma and immediately appreciate how tricky their airway is going to be.
But facial trauma isn't just a tricky intubation. It's an evolving oxygenation, aspiration and extubation problem in a full-stomach trauma patient with distorted anatomy and a shared airway.
The more nuanced details that can get lost in the chaos include:
- How much blood has this person lost?
- What other trauma or burns have they sustained?
- Are they intoxicated?
- Have they also got a traumatic brain injury or intracranial bleed?
- Is their c-spine safe?
- Are they actively haemorrhaging into their airway?
- Have they aspirated already, and are they going to regurgitate on induction?
- What is my plan for extubation?
Let's start with some anatomy
What are the bones of the midface?
- Maxilla
- Zygoma
- Nasal
- Ethmoid
- Lacrimal
- Palatine
- Inferior nasal concha - superior and middle conchae are part of the ethmoid
The naso-orbito-ethmoid complex acts as a sort of crumple zone to help protect the brain from trauma.
Where does midface bleeding arise from?
- Maxillary arteries
- Facial arteries
- Ethmoid arteries
- Nasal mucosa
- Pterygoid venous plexus
Which nerves are particularly susceptible to damage in midface trauma?
- Olfactory - cribriform plate
- Ophthalmic branch of trigeminal - supraorbital foramen
- Maxillary branch of trigeminal - infraorbital foramen
What are the causes of airway obstruction in facial trauma?
- Blood
- Secretions
- Loss of soft tissue tone if unconscious
- Airway distortion
- Tongue - if genioglossus is damaged, the tongue can flop back and obstruct the airway
What signs and symptoms would make you concerned about airway obstruction in facial trauma?
- Visible bleeding
- Dyspnoea
- Stridor
- Drooling
- Odynophagia
- Trismus
- Vocal changes or hoarseness
- Subcutaneous emphysema
- Tracheal deviation
- Burns
Meet René Le Fort

This French surgeon and anatomist decided, in 1901 to be precise, to answer that question that bugs all of us at some point in our lives - exactly how does the human face fall apart under force?
Assembling an array of human cadaver heads, he proceeded to throw them off balconies and hit them with things, before meticulously examining and documenting the results.
He discovered that midface fractures followed predictable patterns, fracturing along lines of weakness, and characterised these into three fracture patterns that we still employ today:
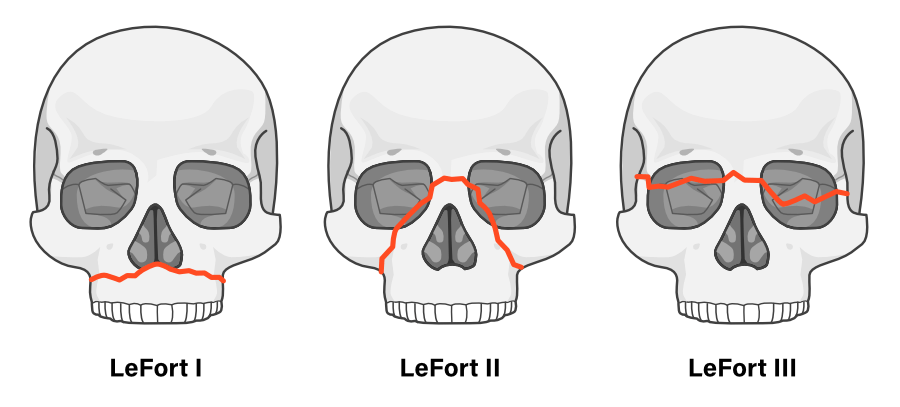
Le Fort I
- Horizontal fracture
- Separates the upper teeth from the rest of the maxilla
This produces a 'floating palate'.
Le Fort II
- Pyramidal fracture
- Maxilla and nasal separation from skull base
Le Fort III
- Most severe
- Transverse fracture through zygomatic arches, lateral orbits and nasal bridge
- Entire midface separates from the skull base
- Total craniofacial dissociation
- May feature dural tear and CSF leak
- Nasal plastic generally contraindicated
What are the signs and symptoms of a basal skull fracture?
- CSF rhinorrhoea
- CSF or blood otorrhoea
- Bilateral periorbital haematoma
- Mastoid ecchymosis
- Haemotympanum
- Eyelid haematoma
- Cranial nerve palsy
Cranial nerve palsies of note:
- CN1 - smell
- CN 2 - visual changes
- CN 7 - facial palsy
- CN 8 - deafness
What are the management for severe bleeding in facial trauma?
- Anterior and posterior nasal packing
- Balloon tamponade
- Reduction of fractures
- Interventional radiology
- External carotid artery ligations
How do I anaesthetise them?
When presented with a patient with severe facial trauma, you need to rapidly assess and decide two things:
- Is induction and intubation required right now?
- If so, how am I going to do this?
This is more tricky than it seems, because there's rather a lot to unpack.
Outline how you would manage a patient with facial trauma
This is a bit of a trick question, because the key is not to be distracted by facial trauma, in the context of potentially catastrophic haemorrhage from somewhere else in the body.
- Start with primary survey as per ATLS approach
- Call for help early, particularly from ENT/Maxillofacial surgeons
- Large bore IV access and fluid resuscitation prior to induction
- Bloods including clotting and crossmatch
- Full monitoring
- Skilled assistance
- Emergency drugs and airway equipment
- Two suction systems ready
- Passive preoxygenation if bag-mask ventilation is risky
- No cricoid if laryngeal injury suspected
- MILS if C-spine concern
- Positioning sat up if safe to do so, can help venous drainage and reduce bleeding
- Videolaryngoscope
- Immediate front-of-neck backup available
What are the indications for intubation in facial trauma?
- Airway compromise - current or impending, such as in burns
- Reduced consciousness - loss of protective airway reflexes
- Uncontrolled facial haemorrhage
- Major anatomical disruption - midface instability can cause sudden airway collapse
- Hypoxia or respiratory distress - need to control ventilation
- To facilitate imaging
- To facilitate safe transfer within or between facilities
- To facilitate damage control surgery
- Severe agitation preventing safe resuscitation
No real surprises here, it's airway protection, ventilatory control and allowing other important things to happen quickly and safely
Remember this is a very dynamic assessment. The airway can change from minute to minute, so have a low threshold to secure it with plastic.
So once you've decided that the poor patient in front of you does indeed require intubation and ventilation, you then have to work out your plan.
What factors, specific to facial trauma, will make intubation more difficult?
The examiners love a 'specific' question in the CRQ paper, which renders many of the generic 'unfamiliar environment, lack of equipment, unstable patient' answers impotent, to test how much you actually understand about this tricky condition.
- Anatomical distortion will make facemask ventilation and preoxygenation more difficult
- Positive pressure mask ventilation may worsen things by forcing air through injured tissue planes causing subcutaneous emphysema or pneumocephalus
- Patient may already have significant trismus
- Temporomandibular joint trauma can affect mouth opening
- Teeth in the airway can be dislodged into the trachea and bronchi
- Supraglottic airway insertion can worsen oropharyngeal trauma
- Blood in airway will affect laryngoscopic view
- Broken teeth can tear the tube cuff
- Airway adjuncts may be contraindicated or make tongue bleeding worse
You can also throw in the old 'often these patients are intoxicated, making setup, positioning and preoxygenation much more difficult'.
Ok so what if I'm not intubating in resus, but they've been booked onto CEPOD by maxfax?
Hopefully the patient has been sufficiently resuscitated, the bleeding has stopped and they're stable, safe and sober enough to have a more controlled induction.
What are your options?
Well it's going to be a shared airway, so to start with you need to have a discussion with your surgeon (MDT input and all that jazz) during which they will almost certainly tell you what sort of tube they need.
- Nasal
- Oral
- Submental
- Retromolar
- Tracheostomy
If they need to wire the jaw or check alignment, then your tube needs to be somewhere other than the mouth, and suspected base of skull fractures make nasal approaches much higher risk.
What is a submental intubation?
- Classic oral intubation
- Surgeon makes submental incision and blunt dissects the floor of mouth
- Tube then passed out through floor of mouth and exteriorised
Here's a splendid video of the procedure.
Here's a tutorial on retromolar intubation.
Awake or asleep?
The answer to this question is found by asking several more questions:
- How difficult do you expect the intubation to be?
- How likely are they to lose their airway if you drift them off to sleep?
- Is an awake nasal tracheal intubation contraindicated?
- Are they going to tolerate an awake intubation?
- Do you have the skillset, equipment and backup necessary for if it goes wrong?
Hopefully the answer to these questions will give you the answer you're looking for.
Useful lines for the viva
“My priorities are oxygenation, suction and a definitive airway, while assuming a full stomach and possible cervical spine injury.”
“I would assess whether this is a stable, cooperative patient with time for an awake technique, or a deteriorating patient needing RSI with a double set-up for front-of-neck access.”
Other things to consider
- Bleeding
- Facial nerve damage
- Throat packs
- Dexamethasone for swelling
- Antibiotics to cover CNS infection
- Temperature management - especially in burns
- Neuroprotective ventilation - if any concern about TBI
Extubation
Remember that if everything goes to plan, then the face you intubated is going to be rather different to the face that eventually gets extubated. This might be done by you at the end of the procedure, or you might choose to keep them asleep on ICU and extubate later.
Factors that will affect this decision:
- Swelling
- Bleeding
- Burns
- Need for other surgery or relooks
- Pain control
- Jaw wiring
What are the complications of a base of skull fracture?
- CNS infection - Meningitis or encephalitis
- Carotid artery dissection
- Cavernous sinus thrombosis
- Pneumocephalus from positive pressure ventilation
- Carotido-cavernous fistula
- CSF fistula
- Pituitary injury
Remember that SIADH is common after major trauma to the head.
Useful Resources and references



More Anaestheasier articles


Primary FRCA Toolkit
While this subject is largely the remit of the Final FRCA examination, up to 20% of the exam can cover Primary material, so don't get caught out!
Members receive 60% discount off the FRCA Primary Toolkit. If you have previously purchased a toolkit at full price, please email anaestheasier@gmail.com for a retrospective discount.

Discount is applied as 6 months free membership - please don't hesitate to email Anaestheasier@gmail.com if you have any questions!
Just a quick reminder that all information posted on Anaestheasier.com is for educational purposes only, and it does not constitute medical or clinical advice.