Scoliosis

Take home messages
- Measure the Cobb angle
- Use an anaesthetic technique that won't mess with spinal cord monitoring
- Think really carefully about positioning
So what is it?
Scoliosis is defined as an abnormal coronal plane curvature with vertebral rotation of the spine and its effects reach well beyond musculoskeletal inconvenience:
- Back pain for hopefully obvious reasons
- Psychological deterioration
- Rib cage deformity inhibits respiratory function, leading to a restrictive respiratory disease
- Cardiovascular dysfunction as a result of increased pulmonary vascular resistance, and for some reason mitral valve prolapse is common
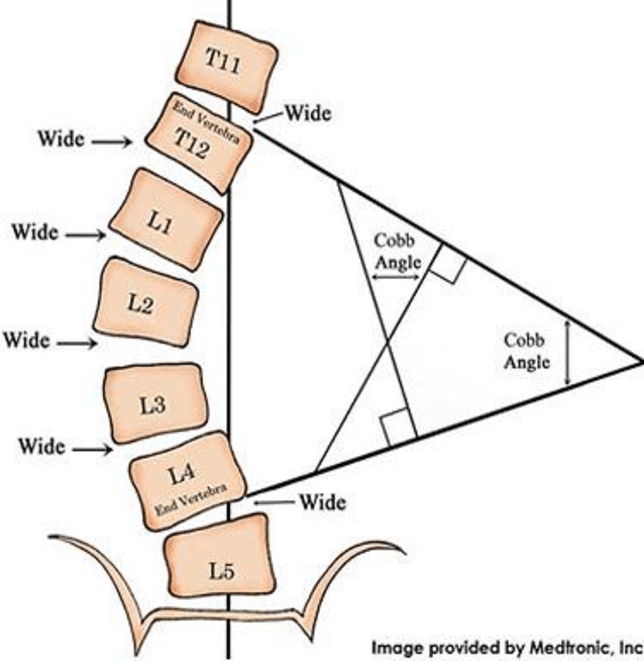
It is generally diagnosed clinically and confirmed radiographically by measuring the Cobb angle, which is the angle subtended by the bodies of the vertebrae at the top and bottom of the greatest degree of curvature, as per the image below.
How is the severity measured?
The Cobb angle is used to determine severity, as this correlates with adverse symptoms:
- 10° needed for diagnosis
- 10°-25° is deemed mild
- 25°-40° is moderate
- 40° is severe and warrants surgical correction
100° almost inevitably leads to respiratory failure, pulmonary hypertension and right heart failure
Briefly summarise the pathophysiology of scoliosis
- Adolescent idiopathic scoliosis is the most common, particularly in females
- In idiopathic scoliosis the underlying cause is unknown, but progression is influenced by growth, muscle imbalance and vertebral rotation
- In neuromuscular and congenital forms, muscle weakness or structural abnormalities impair spinal stability
- This allows the spine to sag against the stabilising ligaments
- If mild or moderate, these curves usually remain stable or even resolve spontaneously
- If severe and untreated, can lead to substantial cardiorespiratory compromise
- This is compounded by underlying conditions such as myopathies and neuromuscular weakness
How is scoliosis classified?
Idiopathic (70%)
- Infantile
- Juvenile
- Adolescent (65 of the above 70%)
Congenital (15%)
- Spina bifida
- Vertebral abnormality
- Marfan’s
- Neurofibromatosis
Neuromuscular (10%)
- Cerebral palsy
- Myopathy
- Syringomyelia
Traumatic
- Fractures
- Radiation
- Surgery
Neoplastic
Infective
- TB
- Osteomyelitis
Degenerative
Clinical features
Visible deformity
- Adam’s forward bend test
- Patient is asked to bend forwards as far as they can to see if spinal curvature remains or straightens out
- This identifies genuine structural scoliosis, rather than curvature caused by poor posture or leg length discrepancy
Pain
- Musculoskeletal back pain
- Radiculopathy
Restrictive lung disease
- Once Cobb angle reaches 65°
- Caused by dysfunction of rib cage mechanics
25 % have mitral valve prolapse
- Linked but unclear why
What are the aims of surgical correction?
What are the aims of surgical management?
- Correction of the curve
- Spinal fusion
- Improve posture
- Prevent respiratory deterioration
- Alleviate pain