Scavenging

This is high up in the rankings of 'driest exam material ever', but it comes up frequently - I was asked about it at both primary and final levels - and it's actually quite important to understand to ensure it gets used properly.
Take home messages
- Scavenging is the removal and safe disposal of waste anaesthetic vapours from the breathing system to avoid contamination of the theatre environment
- This does not stop them from being terrible for the environment
- TIVA is probably slightly better (but still terrible) for the environment
Deep breaths
A large amount of sevoflurane for a short period of time seems to be relatively harmless - we think - for most people, most of the time, for most procedures.
Hence it is so widely used for induction and maintenance of anaesthesia, and seemingly without issue.
However a little bit of sevoflurane for a very long period of time - like every day for an entire career - is less innocuous, and hence we now have scavenging systems in place to reduce the exposure of theatre staff.
Why does it matter?
There is increasing evidence to suggest exposure to sevoflurane and other inhaled agents is best minimised wherever possible, especially if you're not the intended recipient.
What are the adverse effects of chronic exposure to anaesthetic vapours?
- Infertility
- Spontaneous abortion
- Haematological malignancy
- Renal and liver dysfunction
- Cognitive decline
Male anaesthetists exposed to sevoflurane appear to have more female offspring.
The buzzword is 'COSHH' or Control of Substances Hazardous to Health regulations which dictate what the acceptable levels of exposure are. For anaesthetic gases it's calculated as an eight hour time weighted average.
The safe limits are:
- 50 parts per million (ppm) for isoflurane
- 100 ppm for nitrous oxide
- Sevoflurane and desflurane are assumed to be similar to isoflurane, so the same 50 ppm limit is used
Anaesthetic gas scavenging systems are now a legal requirement in theatres.
It doesn't solve the problem
Scavenging systems don't remove the hazardous sevoflurane molecules from existence, they simply remove them from the operating theatre, and by and large - shove them outside.
There they can continue to exert their adverse environmental impacts however they please, so don't get duped into thinking that scavenging systems protect the environment, they don't, they just protect the operating theatre staff.
- Sevoflurane, isoflurane and desflurane are all multiple times more terrible at causing global warming than CO2
- Nitrous also damages the ozone layer (as does anything containing chlorine)
- 5% of the carbon footprint of the NHS is thought to be due to anaesthetic vapours
Although we're not totally to blame for this - most of the nitrous is emitted by Labour ward.
There is technology available that will catalyse conversion of nitrous oxide to O2 and N2 but this isn't widely available in theatres as of yet.
What is GWP100?
- The global warming potential over a 100 year period
- It depends both on how much heat a gas absorbs, and how long it survives in the atmosphere
Sevoflurane is the least terrible as it has the shortest lifespan in the atmosphere, while desflurane lasts the longest, and is therefore the worst.
One bottle of desflurane has the same effect as nearly 900 kg of CO2.
At least they don't directly kill ozone, as neither contains a chlorine atom.
For a bit of perspective:
- All of the inhaled agents produced by the NHS are probably as bad for the environment as one coal power station
- The global warming caused by inhaled anaesthetic agents is less than 0.01% of that caused by global fossil fuel usage
So what do I need?
Well the problem is anaesthetic vapour escaping through the APL and ventilator pressure relief valves, so logically we need to stick a pipe on both of these.
What are the components of a scavenging system?
- Gas collection assembly - uses a 30 mm connector to avoid confusion with other gases and prevent connection to breathing system
- Transfer tubing
- Receiving system or scavenging interface that will depend on the type of system being used
- Disposal assembly
These pipes then simply carry the scavenged anaesthetic gas to the wall and outside.
And that's it.
What types of scavenging are there?
There are three main scavenging systems in regular use - passive, active, and charcoal canisters.
Passive
- Connected to the APL valves
- Essentially a large bore tube that is ducted outside
- Cheap and simple
- Needs access to outside and can be affected by wind
- Risk of obstruction
Active
- Similar to passive but has active vacuum to maintain constant pressure
- Needs to achieve 75 litres per minute with peak flow of 120-140 litres per min
- Some employ an ejector to use the venturi effect to achieve high flows
- Scavenging uses plastic tubing with 30 mm connections to ensure incompatibility with the breathing circuit to avoid accidental connection to the patient
- Scavenging systems need to have a receiving unit with a reservoir and pressure relieving valves to avoid excessive pressure from building up and causing barotrauma
Charcoal canisters
- Cardiff Aldasorber (doesn’t scavenge nitrous oxide)
- replaced every 12 hours
- mobile with no set up cost
- doesn't remove nitrous oxide
- if the canister is heated then the inhalational agents are released back into the atmosphere
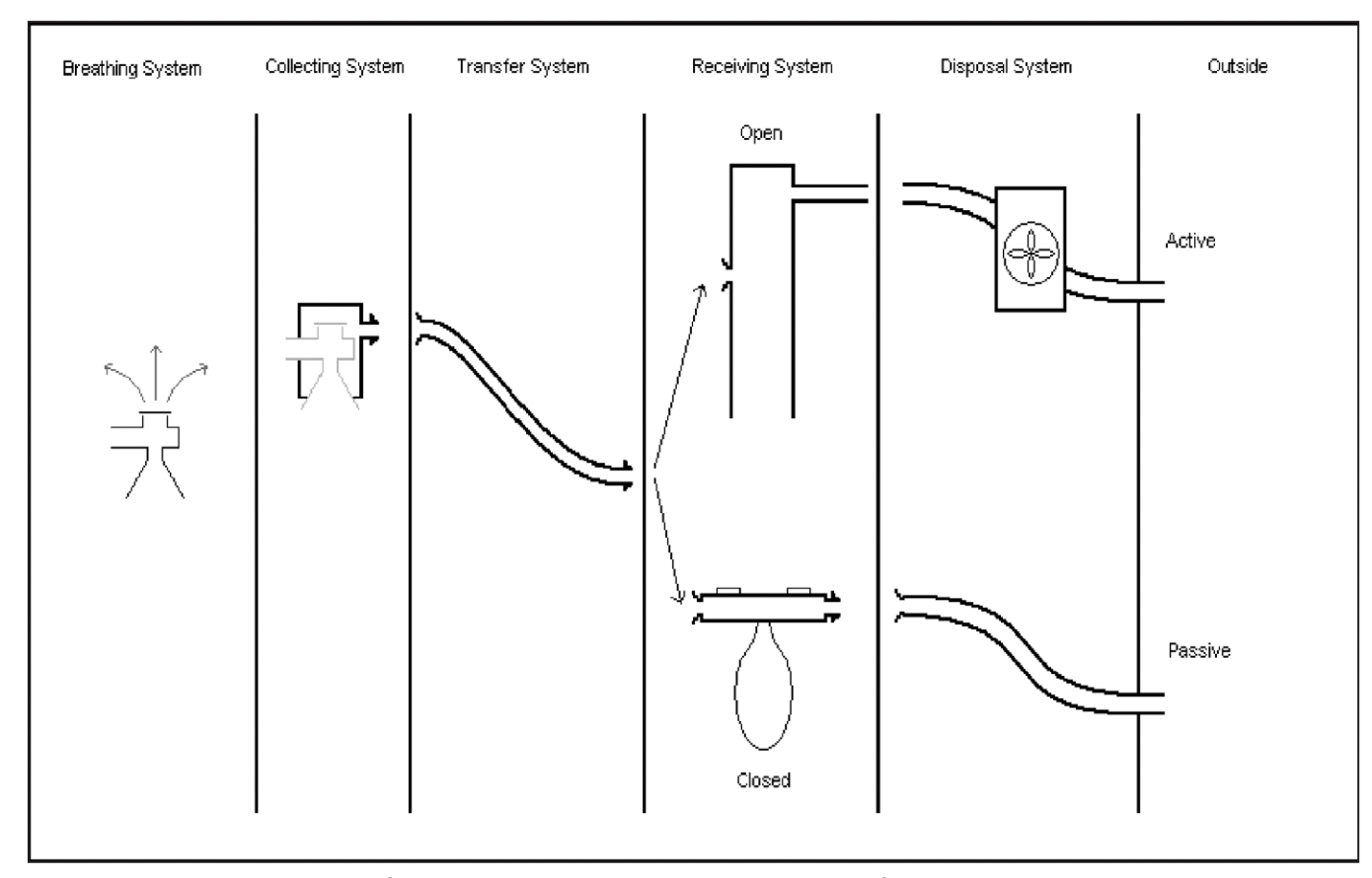
The collecting system
This bit is responsible for gathering up all the waste gases from the breathing circuit (from the APL or relief valves) and stops them being vented out into the room.
- 30 mm connectors (highly examinable material) prevent wrongly connecting them somewhere else in the breathing system
The key here is that you don't want the scavenging attachment to mess up your carefully balanced respiratory dynamics by adding any resistance to the breathing circuit.
The receiving system
You also don't want anything to flow back into the breathing system once it has left, hence there are one way valves incorporated into the scavenging system.
The receiving system acts as a reservoir to prevent the wild swings in pressure in the breathing system from causing mischief.
Receiving systems can be:
- Open
- Closed
An open system is a glorified tube that is open to the atmosphere, acting as a shock-absorber between the disposal system and the breathing system.
A closed system is essentially a bag with positive and negative pressure relief valves, and is not commonly used.
An open system needs an active disposal system to work.
The disposal system
These can be active or passive, and the majority of systems in use in developed regions are active.
- A pump generates negative pressure to draw gas from the receiving system into the disposal system
- The aforementioned open receiving system allows room air to be entrained, and prevents the negative pressure from being transmitted all the way back to the patient
A passive system uses positive and negative pressure relief valves to allow the patient's respiratory effort to push exhaust gas into the aforementioned bag, and then out into the atmosphere.
Here's a useful schematic borrowed from here
Here you can see the scavenging components on a common modern anaesthetic machine.
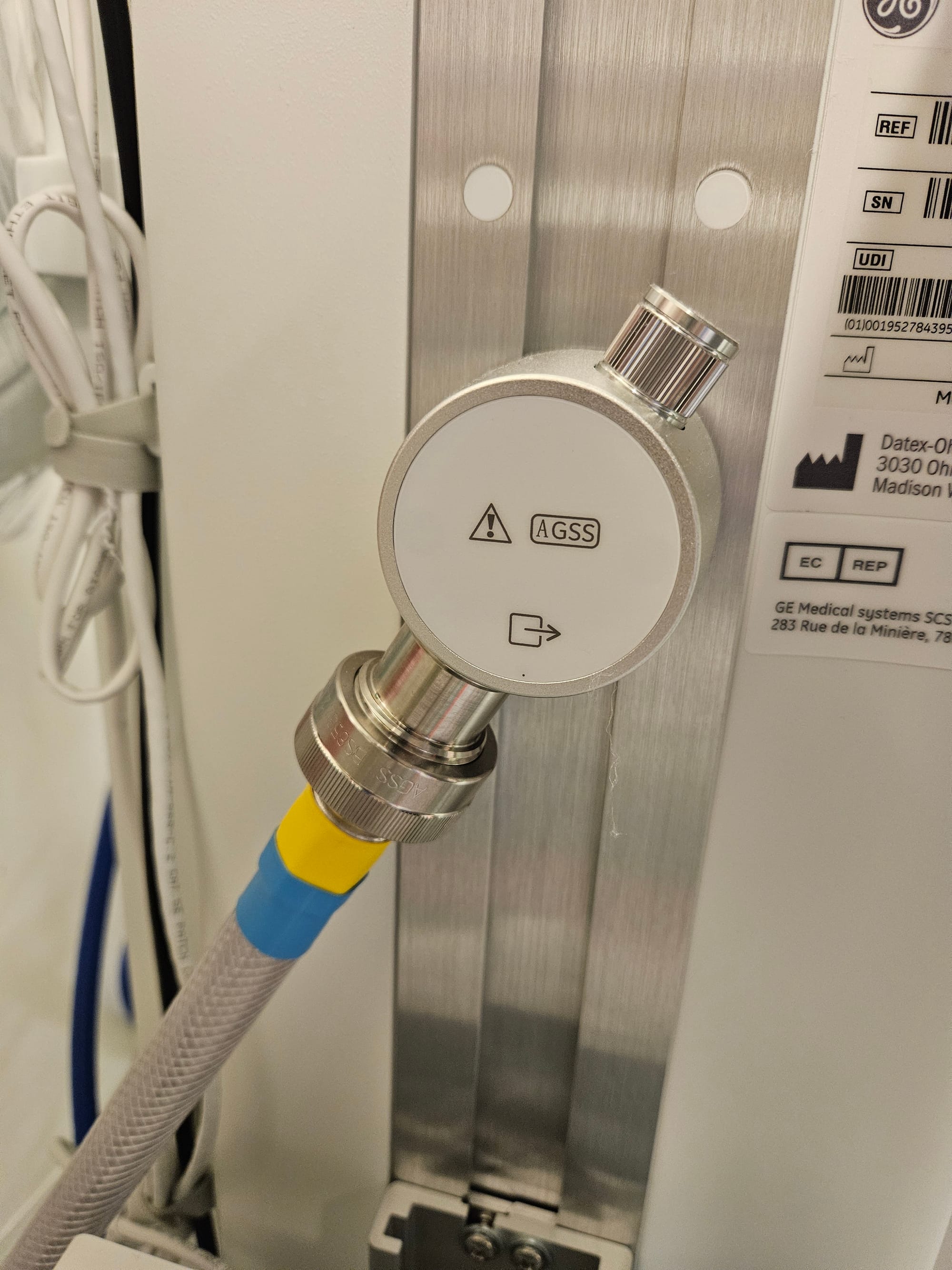



- Note the wide bore meshed translucent tubing that differentiates it from the other medical gas supplies and suction (yellow)
- Note also the completely different connector that prevents misconnection
The Cardiff Aldasorber

You probably won't come across one of these in your day to day practice (we borrowed the image from a veterinary site) but you can still be examined on it, because it's the FRCA and why not?
Here's what you need to be able to regurgitate in an exam scenario:
- Closed system disposable canister
- Uses activated charcoal
- Adsorbs inhaled anaesthetic agents
- Doesn't scavenge nitrous oxide
It is lightweight, simple and convenient to use and doesn't require any active scavenging infrastructure.
However once saturated, the sealed canisters then have to be incinerated at very high temperatures to destroy the volatile agents. If you don't heat them up high enough under controlled conditions, then the vapours will just desorb from the charcoal and float off into the atmosphere.
Is TIVA the answer?
Of course if you don't use any inhalational agents in the first place then the carbon footprint of your anaesthetic is likely to improve to at least some degree.
But when you take into account the environmental cost of
- Manufacturing propofol
- All of the plastic containers, syringes and giving sets
- The harm of renally excreted metabolites entering the water system
- The harm of left over propofol being squirted down the sink
It's not quite as simple, but the general evidence seems to suggest that the longer your case, the better the environmental case for using TIVA, even with all those empty vials and plastic wrappers.
It takes up to 1000°C to fully destroy propofol, hence it should be discarded into the sharps bin for incineration, not down the sink to anaesthetise the fish please.
Syllabus
- PC_BK_25 Suction devices
- PC_BK_26 Scavenging devices
- PC_BK_86 Environmental monitoring: contamination by anaesthetic gases and vapours
Useful resources
Carbon footprint of total intravenous anaesthesia vs. inhalational sevoflurane anaesthesia in adults: a modelling study#anaesthesia #climate #MedTwitterhttps://t.co/IoKOqV6PDw pic.twitter.com/W3Iuet2bGE
— 𝘈𝘯𝘢𝘦𝘴𝘵𝘩𝘦𝘴𝘪𝘢 (@Anaes_Journal) October 15, 2025
References and Further Reading

Primary FRCA Toolkit
If you purchase a copy of the toolkit, you also get six months free membership to your Anaestheasier account as a thank you.

Discount is applied as 6 months free membership - please don't hesitate to email Anaestheasier@gmail.com if you have any questions!
Just a quick reminder that all information posted on Anaestheasier.com is for educational purposes only, and it does not constitute medical or clinical advice.