Remimazolam
Ah man, I just wish there was a version of midazolam that was shorter and cleaner, that I could use for sedation and maybe a bit of general anaesthesia now and again, that doesn't depend on organ function for breakdown and doesn't accumulate.
BOOM.
Wish granted.
Or is it?
Let's take a look.
What are the properties of the ideal sedation agent?
Speed
- Rapid predictable onset
- Easy titration to effect
- Short, context-insensitive offset
- Rapid recovery and discharge
Safety
- Wide therapeutic window
- Readily available reversal agent
- Minimal respiratory depression
- Minimal cardiovascular depression
- Maintained airway reflexes
- Hypoallergenic
- Compatible with other medications
Pharmacokinetics
- Organ-independent metabolism
- Inactive metabolites with no accumulation
Effects
- Anxiolysis
- Anterograde amnesia
- Comfort
- Cooperative sedation
- Analgesia
You can also add in things like 'cheap and easy to manufacture, stable in storage and transit at room temperature, doesn't degrade when exposed to light, compatible with normal plastic giving sets...' etc. etc.
Midazolam and propofol each hit a fair few of these targets, and remimazolam seeks to hit even more, providing the titratability and rapid offset of propofol, the amnesia and anxiolysis of midazolam, the organ independence of remifentanil and all with the safety of a reversal agent too.
CNS-7056
CNS 7056 (now known as remimazolam) hit the news in 2007 after it was found to act in a similar but shorter way than midazolam, with the added benefit of organ-independent metabolism.
It seems to:
- Provide faster offset than midazolam and propofol
- Give deeper sedation than midazolam
- Have a less dose-dependent effect and less pain on injection than propofol
- Cause much less apnoea than remifentanil
Note that it doesn't kick in any quicker than midazolam, it's just shorter in duration of action.
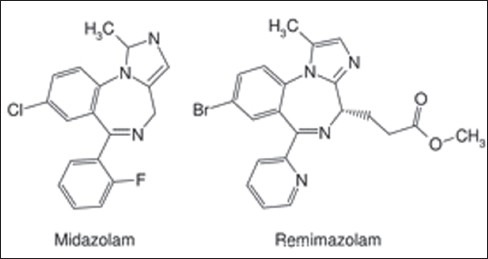
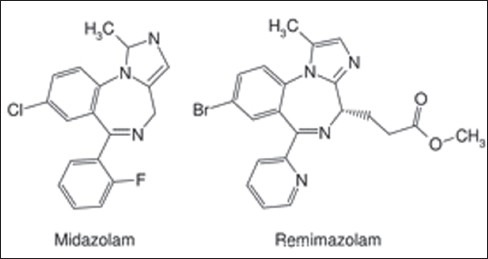
How it looks
As you can see from the image below, it's essentially midazolam with a backpack and a different pair of sunglasses on.
- Ester group side chain
- Chloride switched for bromide
- No fluoride
- Position change for a couple of nitrogens
It's a benzodiazepine
As a quick recap, benzodiazepines act on the GABAa receptor in the CNS, facilitating the opening of a chloride ion channel, leading to chloride influx, hyperpolarisation and therefore reduced neuronal activity.
Benzos have a dose-dependent effect, starting with anxiolysis, then moving through sedation to hypnosis with increasing doses, allowing them to be used as general anaesthetics at much higher doses.
The stats
Brand names
- Byfavo - USA, Canada, Australia, South Korea
- Anerem - Japan
- Ruima - China
- Aptimyda - Europe
Class and presentation
- Ultra short acting Benzodiazepine
- Esterified analogue of midazolam
- Presented as a single use 20mg lyophilised powder
- Reconstituted in 8.2 ml of normal saline to make 2.5 mg/ml solution with pH 2.9-3.9
- Keeps for 48 hours in the fridge once reconstituted
Mechanism and dose
- Positive allosteric modulator of GABAa receptor
- Chloride influx and hyperpolarisation
- Anxiolytic and sedative
Nothing new here.
Dose
- 5 mg IV over 1 minute for procedural sedation
- 2.5 mg every two minutes as needed to top up
- 0.2-0.4 mg/kg for general anaesthesia (off label)
- Studies are ongoing for ICU sedation
I want to know its molecular formula
Of course you do
- C21H19BrN4O2
- Molecular weight 439.3, but the besylate is 597.5
So it's a carbohydrate with a sneaky bromine and a couple of nitrogens right?
Wrong - it's actually this
- [4H-imidazol[1,2-a][1,4]benzodiazepine-4-propionic acid, 8-bromo-1-methyl-6-(2-pyridinyl)-(4S)-methyl ester, benzenesulphonate (1:1)]
So yeah, do with that what you will.
Administration
- IV push
- Incompatible with Ringer's lactate or acetated solutions
Distribution
- Peak sedation 3.5 mins after IV bolus
- 91% protein bound
- Volume of distribution 0.8 L/kg
Metabolism
- Dose-independent hydrolysis by non-specific tissue esterases
- To an inactive carboxylic acid
- Organ-independent clearance
This means at all reasonable doses, you'll see consistent first order metabolism with no accumulation.
Elimination
- Clearance 1.2 L/min
- Half life of 7-8 minutes
- Context sensitive half time of less than 10 minutes after 2 hour infusion
Reversal
- Flumazenil 200 mcg - 500mcg will fully reverse within 2 minutes
Contraindications and warnings
- Known allergy to benzodiazepines or dextran 20 (excipient)
- Severe liver disease is a relative contraindication
- Reduce dose in pregnancy by 30 - 50%
So is it any good?
It seems to be, the following results have been posited:
- Faster recovery with less hypotension and similar success rates to propofol for colonoscopy
- Faster procedure time and much faster recovery compared to midazolam for bronchoscopy
- Similar sedation with much less haemodynamic compromise than propofol for cardioversion
It's probably not useful as a single-shot anxiolytic premed, as it will likely wear off before the procedure has even started. However as a bolus for conscious sedation for a short procedure, where you don't want the cardiovascular instability of propofol or apnoea of strong opioids, it seems to be a great choice.
It may also be a good option for high risk (very obese) patients who are often denied sedation for risk of apnoea and loss of airway.
Here's how benzos work
Sedation top tips
- Always have adequate monitoring and emergency airway equipment available
- Have an answer to 'what is my plan if this patient goes deeper than anticipated?'
- Use capnography to help guide your dosing, not saturations
- When using anything more than minimal sedation, the sedationist should not also be doing the procedure
- Start low and go slow - you can always give more
- Sedation isn't analgesia, so consider short acting opioids or local anaesthetic for painful or stimulating procedures
- BIS or processed EEG is not validated for benzodiazepine or ketamine sedation
- If you're using ketamine, and the patient yawns, that's the time to decide whether you're waking up or giving more
- No driving, machinery or legal decisions for at least 24 hours after sedation (the patient, not you)
What are the different levels of sedation?
- Minimal/anxiolysis
- Moderate/conscious
- Deep sedation
Minimal
- Will respond normally to voice
- Airway, breathing and circulation unaffected
Moderate
- Will respond purposefully to verbal or physical stimulus
- Airway, breathing and circulation usually remain stable
Deep
- May respond purposefully to repeated or painful stimulus
- Airway and breathing support may be needed
- Circulation usually remains stable
Suggest some vaguely sensible doses of different agents you could use, for moderate sedation in a healthy adult
Midazolam
- 0.5 - 1mg IV
- Titrate in 0.5 - 1mg doses every 2 - 3 min
Propofol
- 0.5 mg/kg slowly
- 10 - 20 mg boluses every 1 - 2 minutes
- TCI infusion or 25 - 75 mcg/kg/min titrated to effect
- Avoid large boluses as CVS and respiratory depression
Ketamine
- 0.25 - 0.5 mg/kg
- Consider glycopyrrolate for secretions
- Consider midazolam or propofol for emergence delirium
Dexmedetomidine
- 0.2 - 0.7 mcg/kg/hour
- Can cause bradycardia and hypotension
Fentanyl
- Analgesia rather than sedation
- 12.5 - 25 mcg boluses as needed every 5 - 10 minutes
Remimazolam
- 2.5 - 5 mg IV slow bolus
- 1 - 2.5 mg top ups as needed every 2 minutes
Watch this
How would you sedate a malnourished 30kg child for a three hour scuba extraction from a flooded cave?
- 0.5 mg oral alprazolam
- 20 µg/kg atropine IM
- 5 mg/kg ketamine IM
- 2.5 mg/kg every ≈45 minutes titrated to sedation
- Positive pressure scuba mask
- Prone position to allow buoyancy of mask to hold head up and airway open
Yeah. Mad.
References and Further Reading