Intravenous fluids
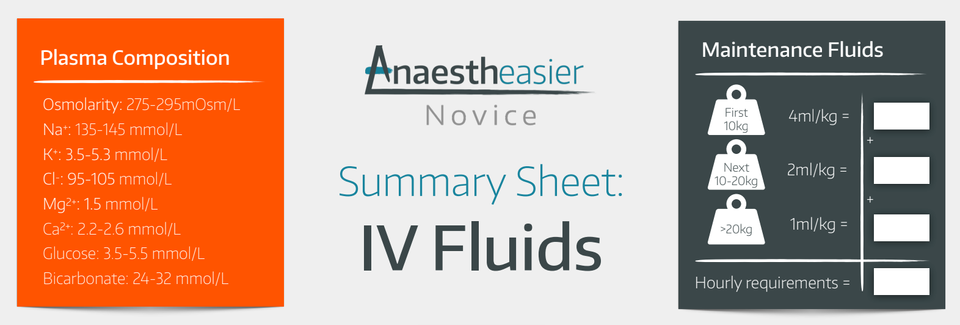
Take home messages
- Decide if you're resuscitating or maintaining
- Review what impact your fluids are having
- Don't give colloids
Crystalloids
Crystalloids are water-based solutions with added solutes (electrolytes or glucose). They differ in their composition, which determines their distribution throughout the body.
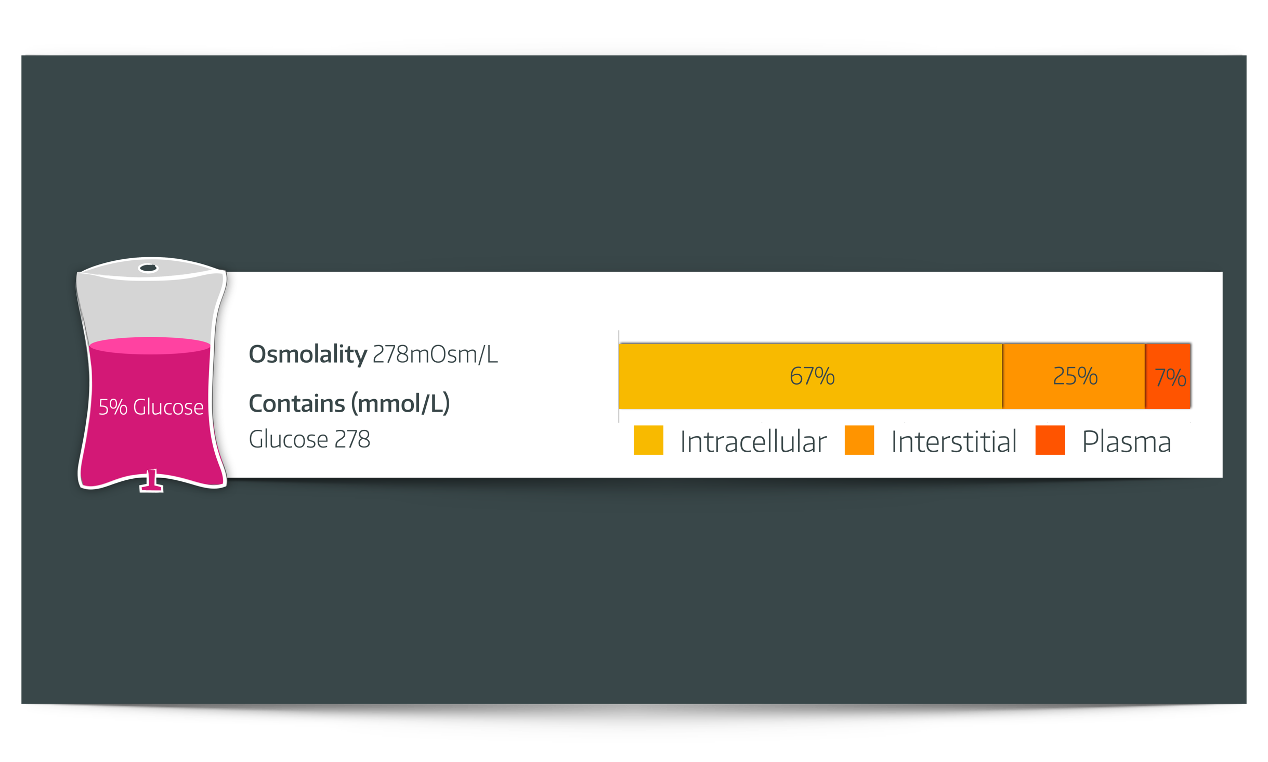
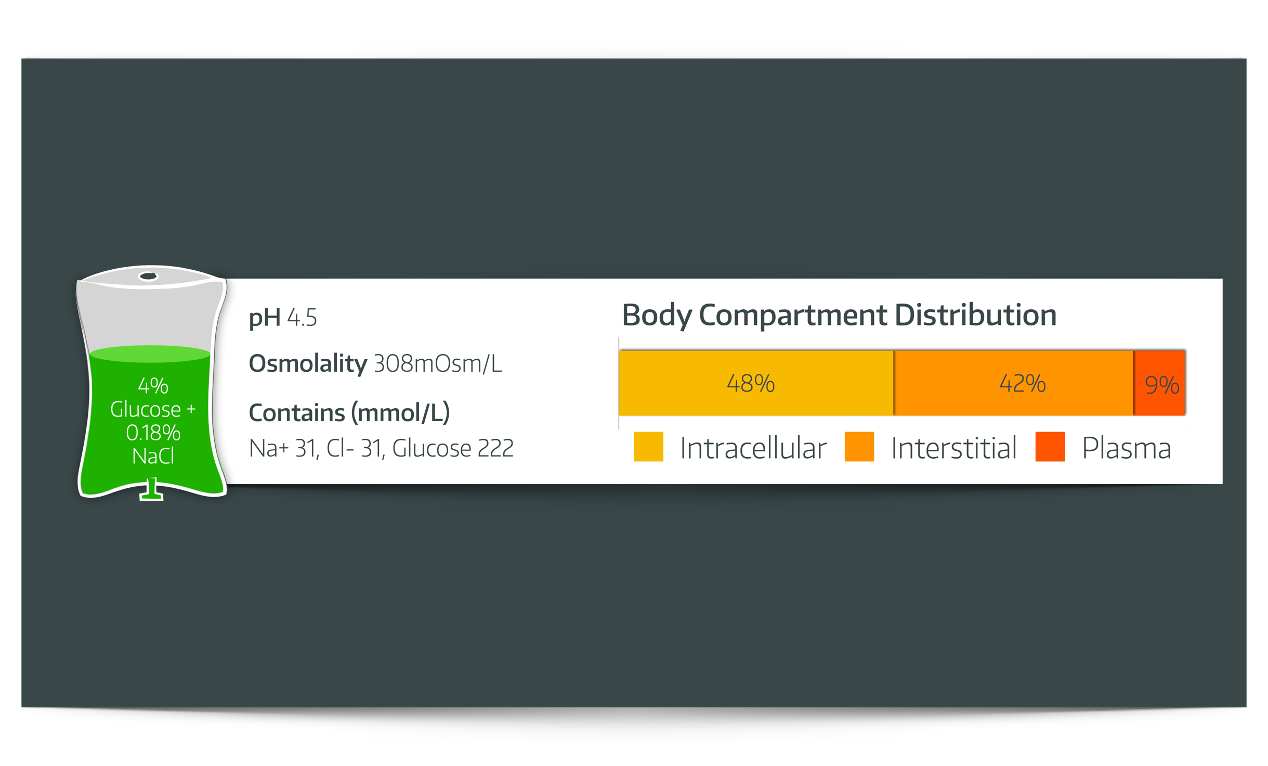
- Once the glucose is metabolised, 5% glucose effectively becomes free water (i.e. not limited to the extracellular space) and so is not suitable for fluid resuscitation as very little remains in the intravascular compartment
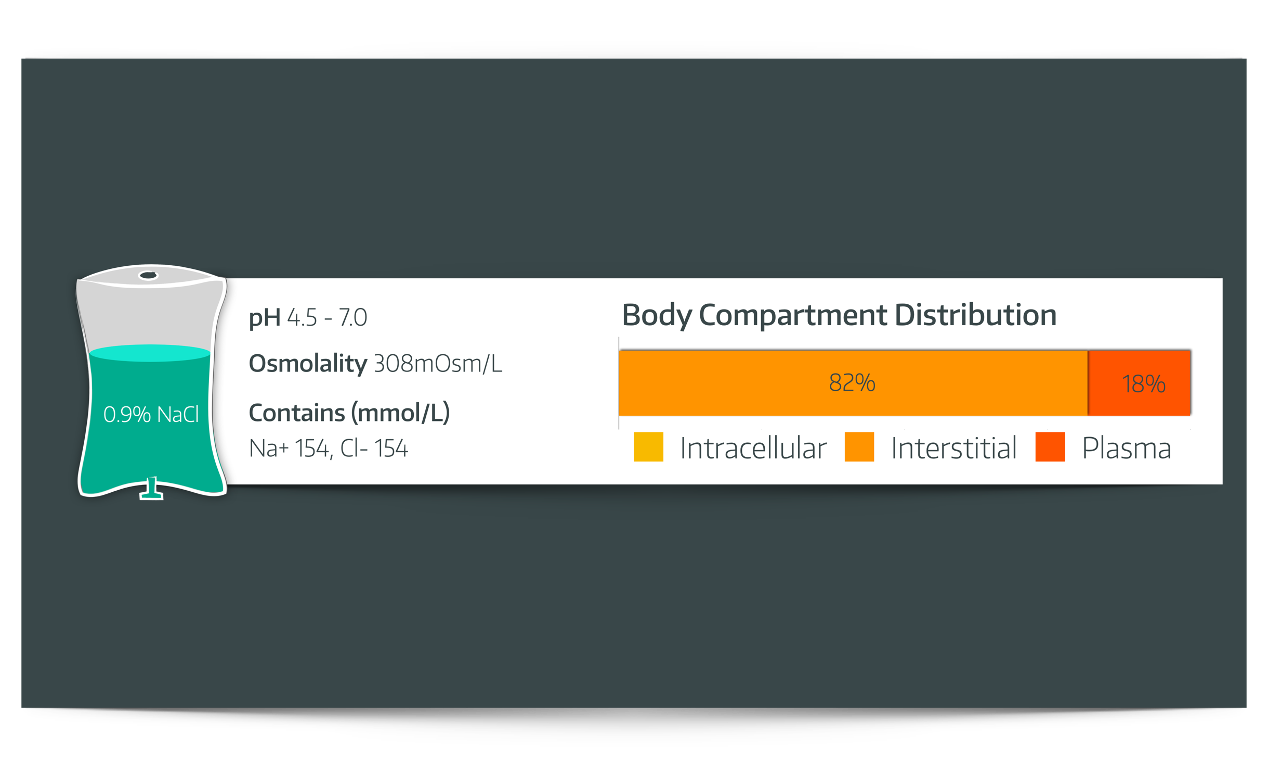
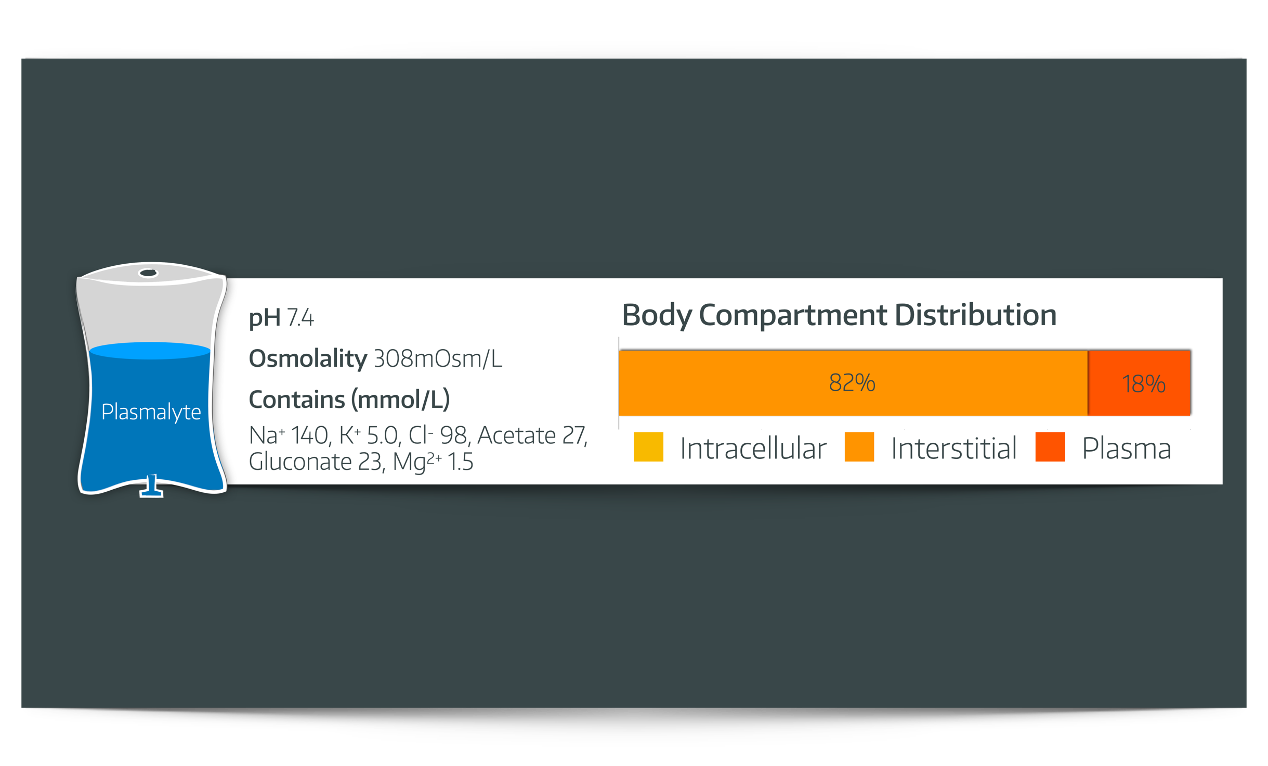
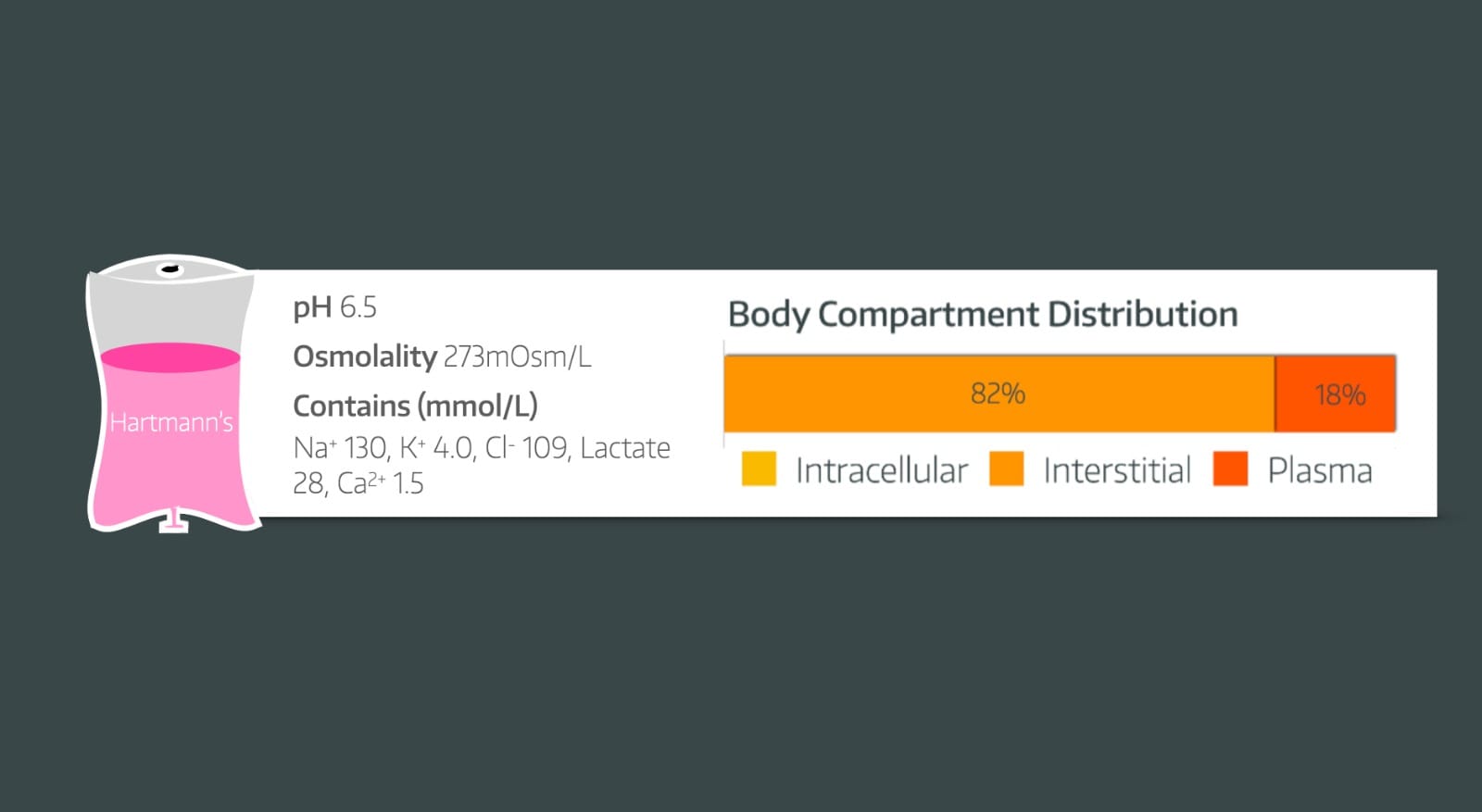
- 'Normal’ Saline and ‘Balanced’ Crystalloids (such as Plasma-Lyte) are retained in the extracellular spaces (in plasma and the interstitium) and so are much more suitable for fluid resuscitation
Normal Saline
5% Dextrose
Plasma-Lyte
Hartmann’s Solution
4% Glucose with 0.18% NaCl
Colloids
Colloids have been popular for their use as plasma volume expanders. This is because they are predominantly retained within the intravascular space (at least initially). They are a crystalloid base with added colloid substance that does not freely diffuse across cell membranes.
Colloids do eventually leak into the interstitium, especially in:
- Sepsis
- Trauma
- Endothelial glycocalyx injury
And can then have the reverse osmotic effect of dragging fluid out of the vasculature with them, which is distinctly suboptimal.
For various reasons (including anaphylaxis and AKI), their use has fallen out of favour.
However, you should be aware of their chemical classification and the pros and cons associated with each.
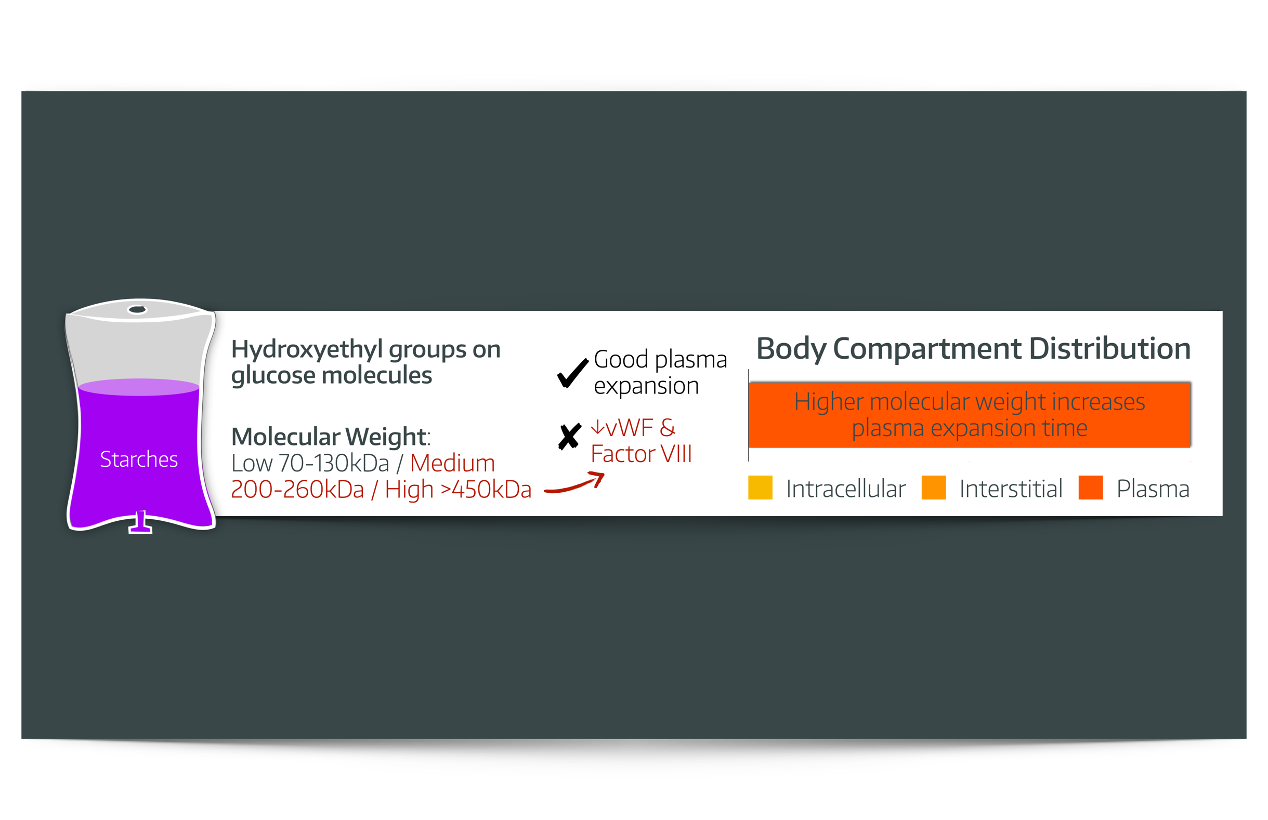
Starches
Dextrans
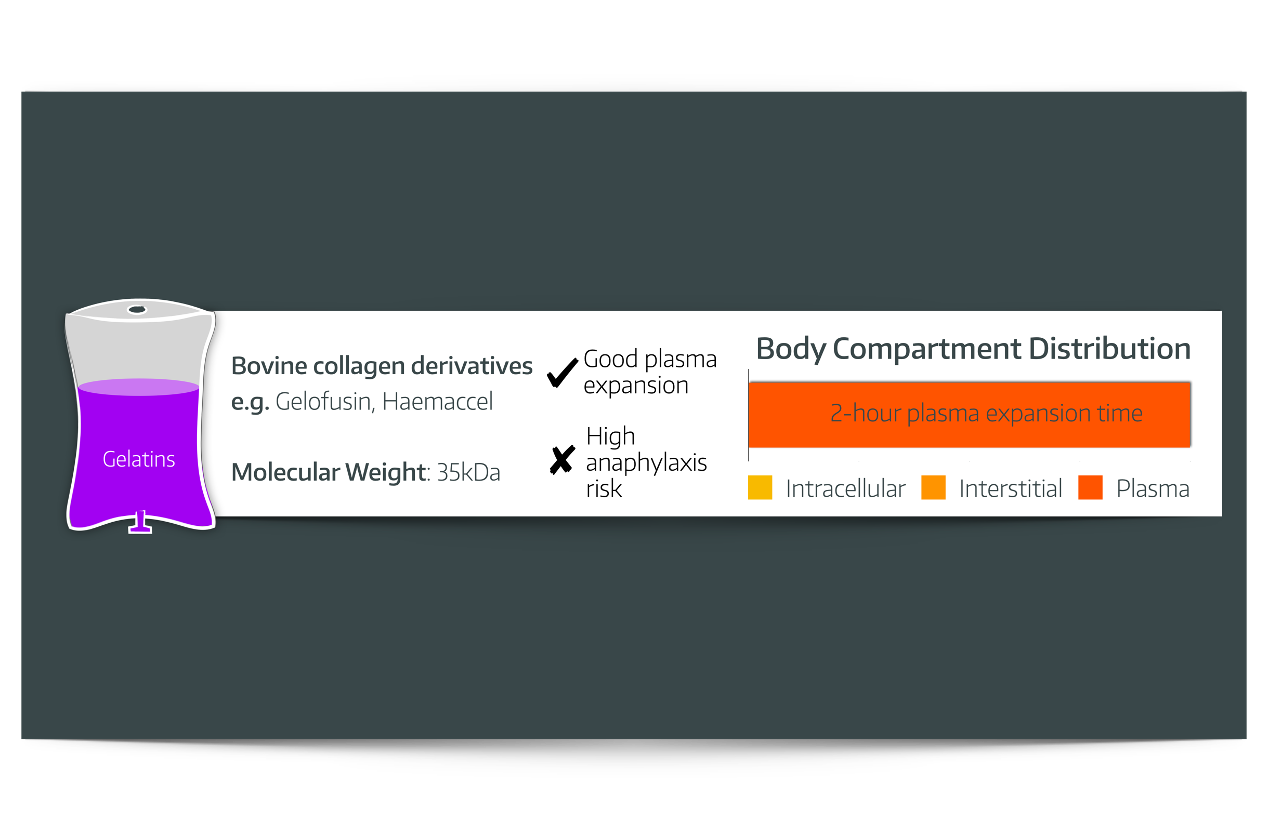
Gelatins
IV fluid Summary Sheet
Our videos
Useful Tweets and resources
We discuss R.O.S.E and the 4 phases of fluid therapy.
— Jonny Wilkinson (@Wilkinsonjonny) May 6, 2023
Resus
Organ support
Stabilisation
Evacuation
We should really only have one phase - resuscitation and then standard maintenance. Period🤷♂️ why go too far and have to remove it..ideal world, I know! pic.twitter.com/N8FdpUZbPK

Primary FRCA Toolkit
Members receive 60% discount off the FRCA Primary Toolkit. If you have previously purchased a toolkit at full price, please email anaestheasier@gmail.com for a retrospective discount.

Discount is applied as 6 months free membership - please don't hesitate to email Anaestheasier@gmail.com if you have any questions!
Just a quick reminder that all information posted on Anaestheasier.com is for educational purposes only, and it does not constitute medical or clinical advice.
Members Area
Test your knowledge!
Member downloads
What proportion of the extracellular fluid compartment is plasma?
- Plasma makes up 20% of the extracellular fluid compartment
- It's 7% of the total body water
How is Plasma-Lyte buffered?
- Acetate and gluconate
Bicarbonate is too unstable in solution as it precipitates with calcium and magnesium, and breaks down during storage.
Acetate and gluconate, conveniently, are not only stable in solution but both are metabolised to bicarbonate after infusion into the patient.
- Acetate is metabolised more quickly than gluconate
- Gluconate reduces the acetate load and side effects
Together they help maintain the strong ion difference required to prevent the hyperchloraemic metabolic acidosis seen with 0.9% NaCl.
What is normal serum osmolality?
- 285-295 mOsm/kg
What is the estimated total body water of a 70kg man?
- 60%
- 42 litres
What are the adverse effects of colloids?
- Due to historical concerns about prion disease transmission, human albumin solution is sourced from screened plasma, primarily outside the UK
- Dextrans are well known to be associated with renal failure
- Anaphylaxis is far more common with colloid use
- Starches are associated with coagulopathy, including reduced Factor VIII and vWF activity