Femoral Nerve Block
Take home messages
- Use ultrasound - it makes onset faster and needs less local anaesthetic
- Remember that bones take innervation from all the surrounding nerves
- You'll need sciatic blockade of some description for knee surgery
Why block the femoral nerve?
Aside from 'for fun' and 'ARCP', patient-centred reasons for blocking the femoral nerve include:
- Analgesia for femoral neck and shaft fractures
- Post operative analgesia (knee replacements, patellar surgery, skin grafts from anterior thigh)
- Post-amputation phantom limb pain
Single shot vs catheter
If you're doing a day case procedure, or the patient is hoping to depart home within 24-48 hours, then a single shot should be adequate (otherwise the procedure is probably not suitable for day case surgery).
If you're anticipating the patient is going to be in for a while, that it's going to be very painful, or there are other issues to think about such as:
- Chronic pain syndromes
- Previous opioid dependance
- Likely to need revision or relook in the same admission
- Palliation for pathological fracture with very short prognosis
Then a catheter is probably a wise choice.
Just remember this will need a dedicated Tuohy needle and catheter, which usually comes a specific regional nerve block set.
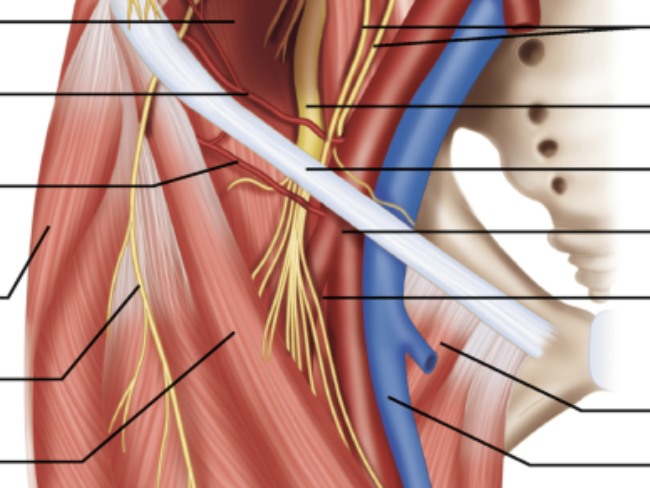
Briefly summarise the anatomy of the femoral nerve
- Originates from L2 - L4 via lumbar plexus
- Emerges lateral to psoas majour
- Passes inferolateral to midpoint of inguinal ligament
- Divides into motor and sensory branches
- Motor supply to quadriceps, sartorius and pectineus
- Sensory supply to anterior and medial thigh and knee
- Sensory supply via saphenous nerve to medial leg, ankle and foot
How to block the femoral nerve
This being anaesthetics, there are multiple ways to skin a nerve and it doesn't really matter how you bathe the nerve in something ending in 'caine' as long as you do it safely.
That being said, the following have historically been the most commonly used approaches.
Femoral Nerve Block
- Targets femoral nerve
- Usually done under ultrasound
- Great for anterior thigh and knee surgery
- Doesn't cover lateral femoral cutaneous nerve or obturator nerve
- Profound motor block
Three-in-One block
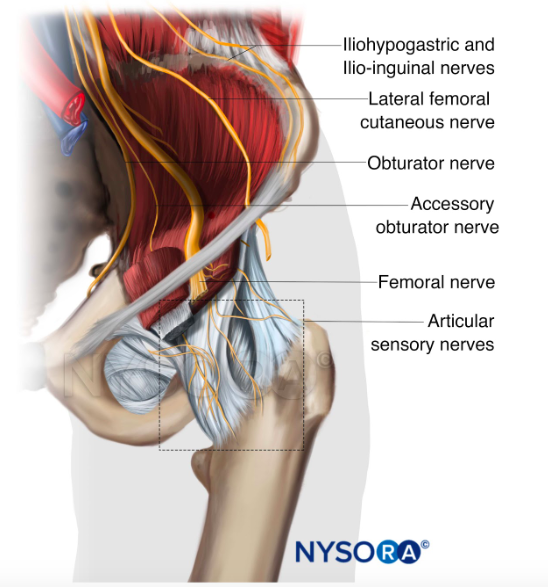
- Targets femoral, obturator and lateral femoral cutaneous nerves
- Injection is essentially at exactly the same site as femoral nerve block
- Higher volume than femoral nerve block
- Pressure applied to femoral nerve distal to injection to encourage proximal spread to cover obturator nerve as well
- Inconsistent cover of obturator, often called '2-in-1' block
Largely superseded by ultrasound guided femoral nerve blocks.
The obturator nerve is primarily motor however it does have some sensory branches to the hip, making it useful to block in hip fracture surgery.
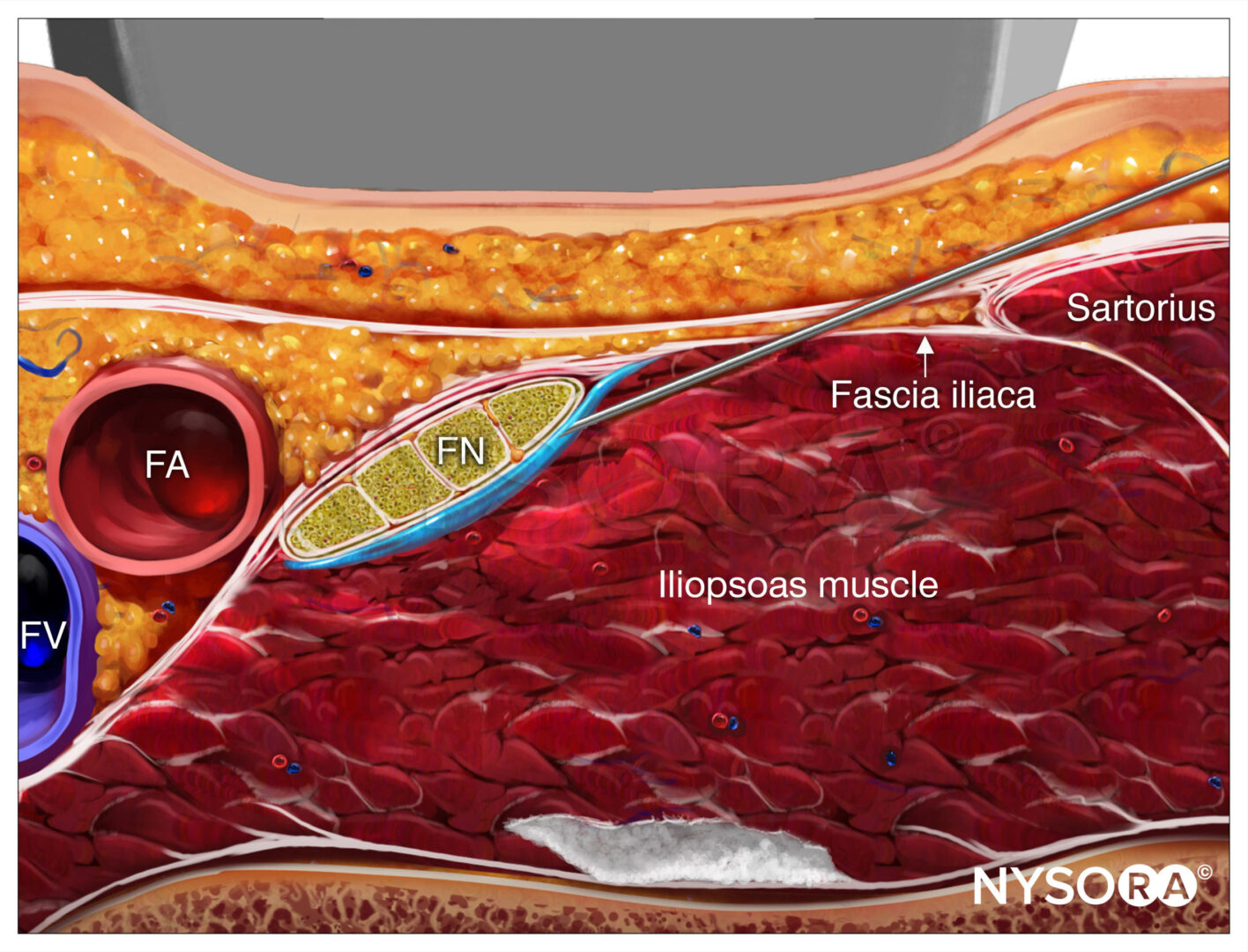
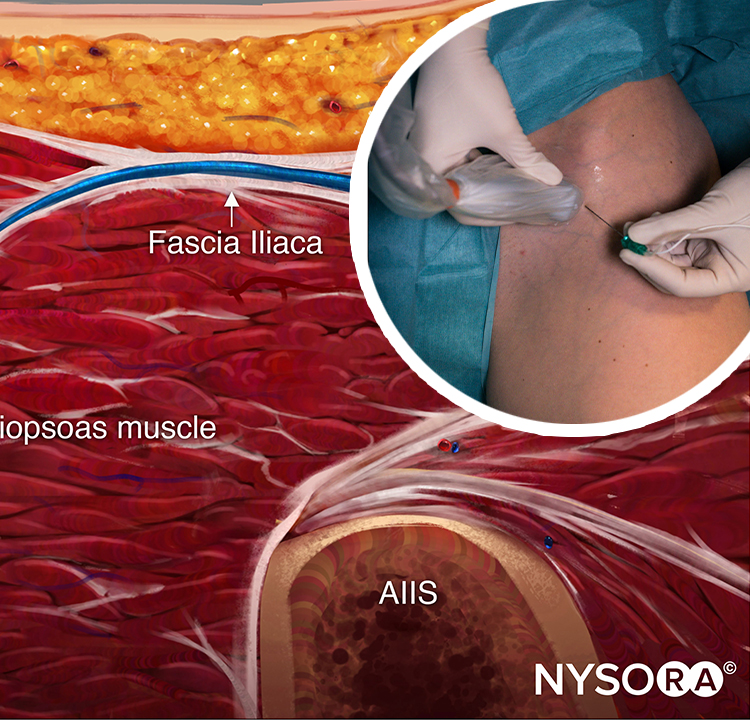
Fascia Iliaca block
The pop pop classic.
- Targets femoral and lateral femoral cutaneous nerves
- Can hit the obturator too if you're lucky
- Large volume of relatively dilute mix injected lateral to femoral artery deep to the fascia iliaca
- Less of a motor block than direct femoral nerve blockade
- Generally considered to be safer as further from important neurovascular structures
Let's not beat around the bush here - they're all basically the same, they just vary ever so slightly with injection location, and they have different volumes of injectate.
As a general rule, the closer you can get the needle tip to the target nerve, the smaller the volume of local anaesthetic required.
The opposite correlation doesn't seem to be true - a bucket of 0.5% placed next to the patient does very little.
There is also the lumbar plexus block and newer PENG block, which we'll discuss later on.
Use Ultrasound
As if you need another excuse to drag the old reliable scanner out - any excuse to play with the toys.
Blocks have historically been performed using a combination of landmarks and nerve stimulators, however the vast majority are now taught and performed under ultrasound guidance, and for good reason.
What are the benefits of using ultrasound?
- Less likely to inject intravascularly
- Smaller volume of drug needed
- Faster onset
An OSCE station
This is an old block that's not used a whole lot these days, but as always, remains highly examinable.
What are the landmarks for performing a 3-in-1 block?
- Anterior superior iliac spine
- Inguinal ligament
- Pubic tubercle
Palpate the ASIS and pubic tubercle. The inguinal ligament that joins these two points.
Mark the midpoint (above the femoral artery). The femoral nerve should be 1cm lateral to this. This is the needle insertion point, and a short blunt needle is advanced to around 3cm depth until paraesthesia felt.
Which nerves are blocked by a 3-in-1 block?
- Femoral nerve
- Lateral cutaneous nerve of the thigh
- Obturator nerve
This is ideally. Much of the time, the obturator isn't covered very effectively, making it more of a '2-in-1 block'
Which nerve roots supply these nerves?
- Anterior primary rami of 2nd, 3rd and 4th lumbar roots
- These supply the lumbar plexus
What volume of local anaesthetic is used?
- 20 - 30 ml
What precautions should be taken during injection?
- Standard AoA monitoring
- Monitor for intravascular injection and ensure intralipid available
- Apply pressure over femoral nerve distal to the injection point, to encourage proximal spread of local anaesthetic
What current is supplied by a nerve stimulator?
- 30 mA at a voltage of 6 - 8 V
- Impulse of <0.3 msec
- Frequency of either 2Hz or 50Hz
Higher frequencies produce pain before lower frequencies.
Which electrode of the stimulator should be applied to the nerve, and which should be placed on the skin?
- Negative applied to nerve as it has a higher current density
- This means 30% less current needed to produce a stimulus
- This helps identify the nerve more accurately
Which nerves are stimulated first, motor or sensory?
- Motor
The GOAT
Here's NYSORA's video, shared with permission.
Here's a useful podcast episode on blocks for knee surgery
Useful Tweets
Part of the process in planning for a peripheral nerve stimulation (PNS) for an Above Knee Amputee suffering with chronic stump pain, a diagnostic Femoral Nerve Block remains an essential step!
— Arun Kalava MD, EDRA (@DrKalava) October 22, 2024
👉 Non-Pulsatile Femoral Artery With an Intravascular Stent
YOUTUBE ➡️… pic.twitter.com/90AV7AF4wU
Incredible #POCUS clip from @TomJelic of a fat embolus sitting at the junction of the femoral and saphenous veins
— Dan Kim (@dan___kim) January 10, 2024
From @CJEMonline "Maintaining screen awareness: the identification of fat embolism with POCUS while performing a nerve block"
🔗https://t.co/pPDrFpbY2k pic.twitter.com/BxOW1OM495
References and Further Reading

Primary FRCA Toolkit
Members receive 60% discount off the FRCA Primary Toolkit. If you have previously purchased a toolkit at full price, please email anaestheasier@gmail.com for a retrospective discount.

Discount is applied as 6 months free membership - please don't hesitate to email Anaestheasier@gmail.com if you have any questions!
Just a quick reminder that all information posted on Anaestheasier.com is for educational purposes only, and it does not constitute medical or clinical advice.