Anaesthesia for Paediatric MRI

Take home messages
- Assume you're not going to be able to access the airway for two hours
- Make sure all your equipment is compatible
- Know where your nearest help and place of safety are
This is an interesting and challenging scenario because you're combining several factors at once:
- Transfer medicine
- Paediatric anaesthesia
- Remote anaesthesia in an unfamiliar environment
- Prolonged procedure with minimal access to airway
- An enormous supercooled electromagnet full of liquid helium that will happily throw an oxygen cylinder through a wall should the occasion arise
So it can be quite tricky.
MRI is cool
As far as medical investigations go, MRI has to be up there in the rankings of 'coolest use of basic physics'.
We won't go into the details here, but you can read our other post on how MRI works here:

Long story short:
- Big magnet
- Hydrogen atoms demonstrating 'spin' align with magnetic field
- Pulses of electromagnetic radiation perpendicular to magnetic field
- Knocks hydrogen atoms out of alignment
- Atoms then 'relax' back into alignment, and fire out radiation of their own
- This is detected by sensors, and an image is generated
That's essentially all you need to be able to say in an FRCA exam.
Why bother using MRI?
MRI provides exceptionally detailed imaging of soft tissues where CT cannot, particularly for the:
- Central nervous system
- Cardiovascular system
- Pelvis
- Liver
- Musculoskeletal system
Its use in diagnostics and interventional procedures has become so integral to modern healthcare that you might even be able to request one on a Saturday evening if you're lucky.
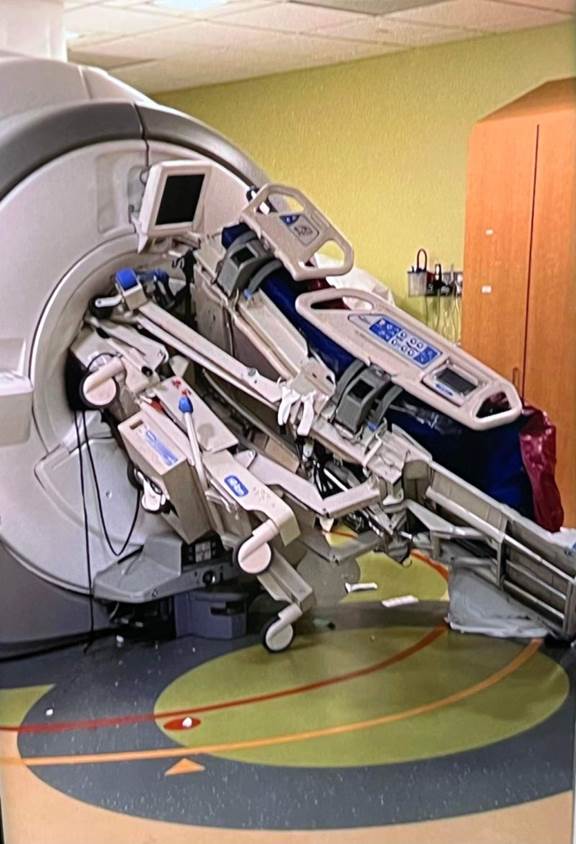
A really big magnet
The earth has a magnetic field strength that is around 0.00005 Tesla, or 0.5 Gauss depending on which system you're using.
This makes it strong enough to deflect solar winds, create auroras, and enables navigation with a compass, but not much else.
Now consider that most modern MRI machines sit anywhere between 1.5 Tesla and 11 Tesla depending on how much money your institution has.
- This produces a magnetic field that is between 30 000 and 150 000 times the strength of the earth's magnetic field
These kinds of magnetic fields will gladly throw oxygen cylinders and ICU beds around the room like a toddler with a bag of skittles.
What are the safety concerns associated with the MRI environment?
- Electromagnet
- Limited access to patient and airway
- Noisy environment
- Risk of equipment incompatibility
How is MRI equipment classified?
- MRI unsafe - can't be used anywhere near a scanner
- MRI conditional - can be used in certain circumstances, up to a certain strength of magnetic field
- MRI safe - no metallic components, can be used in all MRI scanners
What about my metal knee?
- Any ferromagnetic implant is going to heat up and or vibrate
- Non-ferrous metals can still get hot, even if they don't move
- All metal will cause image degradation
- How much of a problem this is will depend on what the implant is and where
Joint replacements, intra-uterine devices, heart valve and shunts are usually fine.
Aneurysm clips, staple and intravascular devices are of variable risk and need to be checked.
Older pacemakers, ocular foreign bodies, cochlear implants and implanted drug infusion pumps are a no no.
Modern pacemakers may be MR conditional - check with the electrophysiologists.
Monitoring
The Association of Anaesthetists recommends that all monitoring equipment is placed in the control room outside of the magnet room.
- Patients have been burned by induced currents in pulse oximeters and ECG leads
- Induced currents will also interfere with interpretation of arrhythmias
- Use of purpose-built MR safe electrodes that convert electrical signals into light sent down fibreoptic cables are much less prone to the effects of an angry electromagnet
- It's not too tricky to get hold of NIBP monitoring that is entirely plastic
- Invasive arterial lines need to be long enough to reach the control room, but short enough to avoid excessive damping
- ETCO2 line length can increase delay in signal change by up to 20 seconds
What are the aims of sedation for MRI?
- Maintain patient's safety and wellbeing
- Minimise pain and discomfort
- Reduce anxiety
- Amnesia
- Control behaviour and movement
This requires careful MDT coordination, and may in some cases require general anaesthesia instead.
What are the risks of using sedation vs general anaesthesia for MRI?
Sedation has:
- Higher failure rate
- More motion artefact
- Variable depth
- Airway less controlled
- Increased hypoxia risk
- Longer setup delays when inadequate
Airway
You can use a supraglottic airway device for MRI scans, however whether you should is a different matter.
Supraglottic airways are used and acceptable for short, low-risk scans with spontaneous ventilation.
As per usual, a tube is preferred if there's any significant aspiration risk, it's a long scan long scan, a difficult airway or need for controlled ventilation.
You'd have a tough time explaining why you didn't use a tube if something bad happened in the scanner and you lost the airway mid-scan.
Once the patient is in the scanner, you are essentially going to have zero access to their airway for the duration of the scan, so make sure you're happy with it before you start scanning.
Where to anaesthetise
As with every anaesthetic, you want to minimise unnecessary steps, including transfer times.
To that end, you'd ideally be anaesthetising your patient as close as possible to the scanning room, but not so close that the scanner causes a problem with your equipment.
Once asleep, with a secure airway, you can think about transferring into the MRI room, and onto the scanning table.
Remember everything needs to be safe in the MRI environment, from your airway to the trolley to the ventilator and the infusion pumps.
Check with your local MRI team whether your equipment is safe to go within the 5 G perimeter or if it needs to stay outside, or fixed to the wall.
What considerations are needed for TIVA pumps?
- You should use MR conditional or MR safe infusion pumps
- Standard pumps need to remain a safe distance from the scanner
- This may require very long infusion lines
- This will increase the resistance for the pump
What about the helium?
Helium is cool when it's in a party balloon or aortic balloon pump. In an MRI scanner it's supercool.
MRI scanners rely on superconductors to maintain such a powerful magnetic field, and to do this they need to be really cold (as in a couple of degrees off absolute zero cold).
To achieve this they use liquid helium, which if allowed to leak out (by accident or by hitting the quench button) then the liquid helium rapidly evaporates and fills the whole room, producing a hypoxic environment that puts everyone who isn't intubated at risk.
This helium should be vented out of the room automatically, and oxygen sensors will alert you to dangerously low O2 levels, but it's something you need to keep in the back of your mind.
References and Further Reading

Primary FRCA Toolkit
While this subject is largely the remit of the Final FRCA examination, up to 20% of the exam can cover Primary material, so don't get caught out!
Members receive 60% discount off the FRCA Primary Toolkit. If you have previously purchased a toolkit at full price, please email anaestheasier@gmail.com for a retrospective discount.

Discount is applied as 6 months free membership - please don't hesitate to email Anaestheasier@gmail.com if you have any questions!
Just a quick reminder that all information posted on Anaestheasier.com is for educational purposes only, and it does not constitute medical or clinical advice.
Anaestheasier® is a registered trademark.